FAQ-MSA/MSP
FREQUENTLY ASKED QUESTIONS
Medicare Set-asides
Medicare Conditional Payments
(Updated 9-1-15)
Overview
This is a series of 99 questions and answers covering Medicare Set-asides, Medicare Conditional Payments, The Centers for Medicare & Medicaid Services (CMS) referrals and other issues related to Medicare Secondary Payer compliance.
Information provided herein is a capsulized version of the more in depth review found in the Author’s original text (and soon to be released Second Edition with release date expected in the Winter of 2015) entitled Practitioner’s Reference Manual To Settlements, Offsets & Set-asides- Second Edition published by Atlantic Law Book Company, West Hartford, Connecticut 06110. The reader is encouraged to visit:
http://www.atlanticlawbooks.com/practionersGuide.htm.
In addition, the answers provided in this Q & A have been derived from information contained in a number of different sources:
- The Centers for Medicare & Medicaid Services’ (CMS) “Workers’ Compensation Medicare Set-Aside Arrangement (WCMSA) Reference Guide” (version 2.3 dated January 5, 2015). This guide can be downloaded at: https://www.cms.gov/Medicare/Coordination-of-Benefits-and-Recovery/Workers-Compensation-Medicare-Set-Aside-Arrangements/Downloads/WCMSA-Reference-Guide-Version-2-3.pdf
- The various Regional Administrative Letters or “Memorandums” issued by The Centers for Medicare & Medicaid Services (CMS) since 2001
- Workers’ Compensation Review Contractor (WCRC)
- CMS WCMSA Operating Rules
- CMS’ web site www.cms.gov
Throughout the Q & A the reader is directed to various sections of CMS’ Workers’ Compensation Medicare Set-Aside Arrangement (WCMSA) Reference Guide (version 2.3 dated January 5, 2015) for additional information on the topic.
Throughout the Q & A the term “beneficiary” is used to indicate an individual who is on Medicare or is otherwise eligible to be on Medicare. This would be the claimant in a workers’ compensation case or the plaintiff in a personal injury liability case.
At present CMS has not issued comprehensive guidelines dealing with Medicare Set-asides (MSA) related to other than workers’ compensation claims. Having said that these guidelines are expected to be released in the near future and most likely will mirror the published guidelines dealing with workers’ compensation claims. Until such time as CMS releases its official guidelines dealing with automobile liability insurance, uninsured and underinsured motorist, no-fault insurance, personal injury protection, homeowner, liability insurance (including selfinsurance), product liability and medical malpractice liability these Q & As will provide the practitioner with guidance in the use of Liability Medicare Set-asides (LMSAs) and related issues.
Disclaimer
The answers provided herein are those suggested by CMS and may not reflect the opinion of Angelo Paul Sevarino, Esq. Where deemed appropriate, “Comment” will reflect the opinion of Angelo Paul Sevarino, Esq. This material is offered for general information only. While every effort has been made to keep this material current there is no guarantee that the answers reflect current CMS opinion, policy or procedures. The reader should always reference www.cms.gov for the most up to date guidance provided by CMS. Additionally this material is not intended as legal advice. Consultation with an attorney experienced in Medicare Set-asides and Medicare Secondary Payer compliance is recommended to address individual issues.
A word about terminology:
Throughout the Q & A the following terminology will apply:
“AWP” average wholesale price
“BCRC” Benefits Coordination & Recovery Center
“Beneficiary” the term used by CMS to indicate an individual who is on Medicare or is otherwise eligible to be on Medicare. This would be the claimant in a workers’ compensation case or the plaintiff in a civil liability case.
“COBC” Coordinator of Benefits Contractor
“COB&R” The Coordination of Benefits & Recovery Center
“CMS” The Centers for Medicare & Medicaid Services
“CRC” Commercial Repayment Center
“GHP” Group Health Plan (whether self-insured or commercial)
“LMSA” Liability Medicare Set-aside
“WCMSA” Workers’ compensation Medicare Set-aside
“WCMSAP” Workers’ Compensation Medicare Set-Aside Portal
“MMSEA” Medicare, Medicaid, and SCHIP Extension Act of 2007
“MSA” Medicare set-aside
“MSP” Medicare Secondary Payer Act
“MSPRC” Medicare Secondary Payer Recovery Contractor
“MSPRP” Medicare Secondary Payer Recovery Portal
“NGHP” Non-Group Health Plan e.g., workers’ compensation, automobile liability insurance, uninsured and underinsured motorist, no-fault insurance, personal injury protection, homeowner, liability insurance (including self-insurance), product liability and medical malpractice liability
“OBRA” Omnibus Budget Reconciliation Act of 1980
“SMART” The Strengthening Medicare and Repaying Taxpayers Act of 2012
“WCRC” Workers’ Compensation Review Contractor
To review a particular question and answer click on the question number below:
Contracting CMS
Statutes, Regulations & Guidelines
Q2. What is the Medicare Secondary Payer Act (MSP)?
Q4. What is the Medicare, Medicaid, and SCHIP Extension Act (MMSEA) of 2007?
Q5. Has CMS issued any guidelines for MSAs?
Q6. What authority does CMS cite for the establishment of a MSA?
Medicare Secondary Payer & Medicare Conditional Payments
Q7. What is a “conditional payment?
Q8. How does the practitioner investigate whether there are Medicare Conditional Payments?
Q9. What is the Medicare Secondary Payer Reporting Portal “MSPRP” ?
Q10. What is the Benefits Coordination & Recovery Center (BCRC)?
Q11. What is the “Medicare Secondary Payer Rights and Responsibilities Letter”.
Q12. What is the Conditional Payment Letter (CPL) and Payment Summary Form(PSF)?
Q13. What is the Conditional Payment Notice (CPN)?
Q14. How is Medicare conditional payment information updated?
Q15. How are disputed Medicare conditional payments resolved?
Q16. What is the “Proof of Representation” authorization?
Q17. What is the “Consent To Release” authorization?
Q18. What is the “Final Settlement Detail Document”?
Q19. What is the “Final Demand Letter”?
Q20. Is a pro-rata reduction for procurement costs allowed to reduce the Medicare recovery amount?
Workers’ Compensation Medicare Set-aside (WCMSA)
Q24. What is a Life Care Plan? How does it differ from a WCMSA analysis?
Q25. What is a Workers’ Compensation Medicare Set-aside (WCMSA)?
Q27. How does CMS define “settlement”?
Q28. What is the difference between a “commutated” and “compromise” settlement?
Q32. Is a WCMSA necessary where the medical component of the case if left open?
Q35. Does a MSA have an effect on Medicaid resources for purposes of eligibility for Medicaid?
Liability Medicare Set-aside (LMSA)
Q37. Does CMS require use of or referral of a LMSA?
Tax implications
Q39. What tax liability does the MSA generate?
MSA Administration
Q40. Who may administrator a MSA?
Q41. What are the MSA administrator’s responsibilities?
CMS Review Criteria and Referral Process
Q43. What are the steps necessary to obtain an approved MSA?
Q44. Who is the Workers’ Compensation Review Contractor (WCRC)?
Q45. Is establishment of a MSA always necessary?
Q46. Does CMS require use of or referral of a WCMSA?
Q51. What are the review thresholds set by CMS?
Q54. What is the referral process for submission of a WCMSA to CMS?
Q55. How does a practitioner register to use the WCMASP?
Q56. What information is needed for WCRC review?
Q57. What are the most frequent reasons for development requests by BCRC or WCRC?
Q59. What happens after a WCMSA has been reviewed?
Q60. How does the submitter check the status of a WCMSA Referral?
Q61. Once the WCMSA has been approved by CMS what is CMS’ subsequent role?
Disbursements from the MSA
Q65. What disbursements may be made from the WCMSA?
Q69. How are prescription drug charges paid from the WCMSA?
Q70. What if there is a dispute as to whether the MSA pays?
Duration, Depletion & Termination of the MSA
Q71. May the MSA contemplate only a finite period of time?
Q72. How may the MSA be reduced or terminated??
Q73. What is a “temporary depletion” of a structured MSA?
Q74 What is a “Residual Secondary Payment”?
Valuation, Calculation & Reduction of the MSA
Q77. What types of investment vehicles may be used to house the MSA?
Q78. Is the MSA indexed to account for inflation or reduced to present cash value?
Q81. Can a MSA be established by lump sum funding?
Q82. Can a MSA be established by use of a structured arrangement?
Q83. How do you calculate the funding when using a structured MSA?
Q84. Are there special rules for pricing implantable devices when included in a MSA?
Prescription Drugs & Medicare Part D
Q85. What is WCRC’s prescription drug review process?
Q86. What is the definition of a “covered” Medicare Part D Drug?
Q93. What is CMS’ policy regarding the expiration of drug patents?
Q94. What is CMS’ policy regarding “off-label” use?
Q95. What is CMS’ policy regarding a carrier’s reliance on utilization review?
Conflicts between State & Federal Laws
Q97. Does CMS recognize or honor any State specific statutes that conflict with CMS policy?
Ethical Considerations
Q98. What are an attorney’s ethical obligations to the client in the context of a MSA?
Disclaimer
The answers provided herein are those suggested by CMS and may not reflect the opinion of Angelo Paul Sevarino, Esq. Where deemed appropriate, “Comment” will reflect the opinion of Angelo Paul Sevarino, Esq. This material is offered for general information only. While every effort has been made to keep this material current there is no guarantee that the answers reflect current CMS opinion, policy or procedures. The reader should always reference www.cms.gov for the most up to date guidance provided by CMS. Additionally this material is not intended as legal advice. Consultation with an attorney experienced in Medicare Set-asides and Medicare Secondary Payer compliance is recommended to address individual issues.
A1. Contacting CMS depends on which department of CMS inquiry is being made.
To report a new workers’ compensation occurrence to the BCRC:
(for Medicare conditional payments)
Any workers’ compensation claim that is ready for settlement should be reported by telephoning the Benefits Coordination & Recovery Center (BCRC). Written notice can also be utilized, however this will slow down the process and is not encouraged. Note: This reporting process is NOT the reporting process that is required under the Medicare, Medicaid, and SCHIP Extension Act (MMSEA) of 2007. See Q & A 4.
By telephone: 1-855-798-2627 or TTY/TTD 1-855-797-2627.
By written notice addressed to:
Medicare-Medicare Secondary Payer
MSP Claims Investigation Project
P.O. Box 138899
Oklahoma City, OK 73113-8897
Notice to the BCRC must contain the following information:
- a. Injured person’s name, address, telephone number, Social Security number(SSN) or Health Insurance Claim number(HICN), and date of birth
- b. Injured person’s attorney’s name, address and telephone number
- c. Employer (WC claims only) name and address.
- d. Insurer’s name, address, telephone number and claim number
- e. Insurer’s attorney’s name, address and telephone number
- f. Date of injury
- g. Body part(s)/system(s) related to the incident
- h. Related ICD-9/10 codes (preferred but not mandatory)
- i. Description of how injury occurred or illness was contracted
Reference additional information at: WCMSA Reference Guide, §2.2
For WCMSA inquiries:
If the practitioner is in need of general information regarding the WCMSA referral process contact:
Benefits Coordination & Recovery Center (BCRC)
P.O. Box 138832
Oklahoma City, OK 73113
1-855-798-2627 or TTY/TTD 1-855-797-2627
Note: This mailing address is for general information and not for submission of a WCMSA proposal or to report a workers’ compensation occurrence.
Referring the WCMSA to BCRC by Hard Copy or CD
If the practitioner has submitted a WCMSA but has not yet received an acknowledgment letter from the BCRC contact:
Benefits Coordination & Recovery Center (BCRC)
P.O. Box 138832
Oklahoma City, OK 73113
1-855-798-2627 or TTY/TTD 1-855-797-2627
If the practitioner has submitted a WCMSA and has received an acknowledgement letter from the BCRC contact:
WCMSA Proposal/Final Settlement
P.O. Box 138899
Oklahoma City, OK 73113-8899
If the practitioner has submitted a WCMSA via the WCMSAP portal and has received an acknowledgment letter from the BCRC log in to the WCMSAP portal to check the status of the WCMSA proposal.
A list of CMS’ Regional Offices and the states they service along with contact information can be found at the CMS web site: www.cms.gov/RegionalOffices.
If the practitioner cannot get an answer from one of the above CMS may be contacted by mail at the following address:
Department of Health & Human Services
Centers for Medicare & Medicaid Services
7500 Security Boulevard
Baltimore, Maryland 21244-1850
Statutes, Regulations & Guidelines
A2. On 12-5-80 the Omnibus Budget Reconciliation Act of 1980 (OBRA) established the Medicare Secondary Payer provisions (MSP) codified in Section 1862(b)(A)(ii) of the Social Security Act (42 U.S.C. §1395y(b)(2), 94 Stat. 2599 , Pub L. No. 96-499, §953; applicable regulations are found at 42 C.F.R. 420 et seq.)
Since Medicare’s inception in 1965 workers’ compensation coverage has always been a primary payer to Medicare. The primary purpose of the passage of the MSP was to make Medicare a secondary payer to other insurance in addition to workers’ compensation. This included group health plans (whether self-insured or commercial), automobile liability insurance, uninsured and underinsured motorist, no-fault insurance, personal injury protection, homeowner, liability insurance (including self-insurance), product liability and medical malpractice liability.
As of February 1, 2014 the primary entity responsible for enforcement of the MSP provisions is The Coordination of Benefits & Recovery Center (COB&R). Within the COB&R are two agencies: (a) the Benefits Coordination & Recovery Center or “BCRC” who has the responsibility for NGHP conditional payment reconciliation, and (b) the Commercial Repayment Center (CRC) who has responsibility for GHP conditional payment reconciliation. The BCRC was formerly two distinct entities e.g., the Coordination of Benefits Contractor or “COBC” and the Medicare Secondary Payer Recovery Contractor or “MSPRC”.
Effective October 2015 the CRC will assume responsibility for the recovery of conditional payments where CMS is pursuing recovery directly from a liability insurer (including a self-insured entity), no-fault insurer or workers’ compensation entity as the identified debtor. Beneficiaries and their attorneys will continue to work with the BCRC where CMS is pursuing recovery from the beneficiary.
The BCRC consolidates the activities that identify the group health, workers’ compensation or liability benefits available to the beneficiary, support the collection, management, and reporting of other insurance coverage for the beneficiary and coordinate the payment of Medicare submitted medical services or prescription drug bills so as to prevent mistaken payment by Medicare of Medicare benefits. The BCRC does not directly process Medicare claims.
The MSP also created the concept of “conditional payments”, as well as, Medicare’s rights to recovery of such payments. The responsibility for monitoring and resolving conditional payments rests with the BCRC. See Q & A 7 for a discussion of conditional payments.
The BCRC is responsible for any action to recover a conditional or “mistaken” (see Q & A 7 for a discussion of “mistaken” payment) Medicare payment(s). The BCRC monitors the various payments made to the beneficiary and issues demand letters (see Q & A 19) for repayment to any parties who may be obligated to repay Medicare e.g., employer, insurer, third party administrator, plan or other plan sponsor. If the BCRC does not receive repayment or a valid documented defense in response to its inquiry the BCRC may refer the debt to the Department of the Treasury for the Treasury Offset Program and other cross-servicing activities pursuant to the Debt Collection Improvement Act of 1996 (110 Stat. 1321, Pub l. 104-134, 31 C.F.R. 285).
The essence of the MSP is to prevent the shifting of responsibility for payment of work or accident related medical services and prescription drug charges from a primary payer to Medicare. The MSP provides that Medicare may not make payment on behalf of a beneficiary for medical services or prescription drug charges where payment has been made or can reasonably be expected to be made promptly under (1) a workers’ compensation law or plan of the United States or a State or (2) under a liability policy (including a self-insured plan) or automobile no-fault coverage or (3) group health policy. If one of these primary plans does not pay or cannot be expected to pay promptly Medicare may make the payment “conditionally”
Note: Medicare through the MSP and CRC will seek recovery from both group health plans (GHP) and non-group plans(NGHP). The discussion contained herein relates only to the NGHP plans.
Under the MSP Medicare has a priority right of recovery from the primary payer, as well as, from parties in receipt of third party payments such as a beneficiary, provider, supplier, physician, attorney, state agency or private insurer pursuant to 42 CFR 411.25(g). This recovery can result in Medicare recovering the entire settlement amount to satisfy its recovery claim.
Medicare benefits are secondary to benefits payable by a primary payer even if State law or the primary payer states that its benefits are secondary to Medicare benefits or otherwise limits its payments to Medicare beneficiaries.
Medicare regulations specify in great detail the basis for the amount of any Medicare secondary payments. A Medicare secondary payment is the lowest of the actual charge by the supplier, the amount that Medicare would pay if the medical services were not covered by a primary payer, or the higher of the Medicare fee schedule, reasonable charge or other amount payable under Medicare.
Comment: Note that this is not a “super-lien” as some are fond of calling it but rather a “right of recovery”. In the former the practitioner would have an obligation to “protect” Medicare’s interest. Rather what the law requires is that the practitioner “considers” Medicare’s interest. The practitioner’s obligation is to protect his or her client’s rights.
A3. The Strengthening Medicare and Repaying Taxpayers Act of 2012 (SMART) H.R. 1845 passed in 2012 and was signed by President Obama on 1-10-13. SMART made significant improvements to the Medicare conditional payment reconciliation process ( see Q & A 7-23) and modified certain provisions of the Medicare, Medicaid, and SCHIP Extension Act (MMSEA) of 2007 (see Q & A 4) which simplified the current online web portal process for calculating Medicare conditional payment reimbursements thereby making the process more efficient and cost effective.
SMART does NOT impact Medicare Set-asides as it ONLY applies to Medicare conditional payments and certain provisions of the MMSEA (reporting law). Some parts of SMART will not be implemented for 18 months. Regulations for implementing the Act have yet to be promulgated.
Chief among the Act’s provisions are:
Section 201
a. 42 U.S.C. §1395y(b)(2)(B)(vii)((I) will require CMS to issue a final demand for repayment of conditional payments before a settlement, judgment or award in claims involving liability, no-fault or workers’ compensation claims. 42 U.S.C. §1395y(b)(2)(B)(vii)(I) further provides that beginning no sooner than 120 days before the reasonably expected date of a settlement, judgment, award, or other payment, the beneficiary or insurance carrier may provide notice of such settlement, judgment, award, or other payment to CMS (through the web portal) that a payment is reasonably expected and the expected date of such payment. Author’s Comment: this provision does not replace existing reporting obligations by the carrier under the MMSEA.
b. under 42 U.S.C. § 1395y(b)(2)(B)(vii)(II):
- (aa) CMS is mandated to “update the information on claims and payments on such website in as timely a manner as possible but not later than 15 days after the date that payment is made.” In addition the claim information “shall include provider or supplier name, diagnosis codes (if any), dates of service, and conditional payment amounts”
- (bb) provide information accurately so as to identify those claims and payments that are related to a potential settlement, judgment, award or other payment
- (cc) the website provides a method for the receipt of secure electronic communications with the individual, representative, or plan involved.
- (dd) provide via the web portal information with an official time and date that the information is transmitted
- (ee) the website shall permit beneficiary (and any authorized representative) and insurance carrier to download a “statement of reimbursement amounts” on payments for claims relating to a potential settlement, judgment, award or other payment. Author’s Comment: this appears to replace the conditional payment letter and payment summary form.
c. 42 U.S.C. § 1395y(b)(2)(B)(vii)(III) provides that if an individual or other beneficiary or insurance carrier with the consent of the beneficiary obtains a statement of reimbursement amount from the website during the “protected period” and the related settlement, judgment, award or other payment is made during such period, then the last statement of reimbursement amount that is downloaded during such period and within 3 business days before the date of the settlement, judgment, award or other payment shall constitute the final conditional amount subject to recovery related to such settlement, judgment, award, or other payment.
“Protected period” is defined at 42 U.S.C. § 1395y(b)(2)(B) (vii)(V) as commencing from the date of notice to CMS and extending for 65 days, except such period may be extended by CMS for a period of an additional 30 days if CMS determines that additional time is required to address claims for which payment has been made. The protected period shall also be extended and shall not include any days for any part of which CMS (regulations not yet promulgated) determining that there was a failure in the claims and payment posting system and the failure was justified due to “exceptional circumstances” e.g. system failure(s) due to consequences of extreme adverse weather (loss of power, flooding, etc.); security breaches of facilities or network(s); terror threats; strikes and similar labor actions; civil unrest; uprising or riot; destruction of business property (as by fire, etc.); sabotage; workplace attack on personnel; and similar circumstances beyond the ordinary control of government or private section officers or management, which are estimated to not exceed more than 1% of the repayment obligations.
d. Under 42 U.S.C. § 1395y(b)(2)(B)(vii)(IV) the beneficiary and any entity with the consent of the beneficiary, may dispute any entry in the statement of reimbursement amount. The beneficiary or representative must then provide documentation explaining the discrepancy and a proposal to resolve such discrepancy. Within 11 business days after the date of receipt of such documentation CMS shall determine whether there is a reasonable basis to include or remove claims on the statement of reimbursement. If CMS does not make such a determination within the 11 business day period then the proposal to resolve the discrepancy shall be accepted. If CMS determines within such period that there is NOT a reasonable basis to include or remove the claim on the statement of reimbursement, the proposal shall be rejected. If CMS determines within such 11 business day period that there is a reasonable basis to conclude there is a discrepancy then CMS must respond in a timely manner by agreeing to the proposal to resolve the discrepancy or by providing documentation showing with good cause why CMS is not agreeing to such proposal and establishing an alternate discrepancy resolution. In no case shall the process be treated as an appeals process or as establishing a right of appeal for a statement of reimbursement amount and there shall be no administrative or judicial review of CMS’ determinations.
e. Establishes a limited right of appeal for insurance companies and the self-insured employer (this does not apply to beneficiaries) applicable should CMS attempt a recovery claim against a qualifying primary payer. Under 42 U.S.C. 1395y(b)(2)(B)(viii) the Act requires CMS to promulgate regulations establishing a right of appeal and appeals process with respect to any determination for a payment made for an item or service for which CMS is seeking to recover conditional payments from an applicable plan that is a primary plan. The beneficiary shall be notified of the plan’s intent to appeal such determination. Note, the deadline to implement this provision can be extended by CMS 1 or more periods of up to 1 year each if extension is necessary to protect patient privacy or protect the integrity of the MSP program.
In response to Section 201(e) CMS proposed a new regulation effective November 12, 2013 42 CFR 405 entitled “Medicare Program: Right of Appeal for Medicare Secondary Payer Determination Relating to Liability Insurance (including Self-Insurance), No Fault Insurance, and Workers’ Compensation Laws and Plans” was proposed. The proposed regulation revision amends 42 CFR 405 provisions and added some new ones to include appeals for applicable plans where Medicare is pursuing recovery directly from the applicable plan and provides.
- 1. adding amending 42 CFR 405.900 by revising paragraph (a) to add section 1862(b)(2)(B)(viii) requiring an appeals process for applicable plans when Medicare pursues recovery directly from the applicable plan;
- 2. add to §405.902 a statutory definition of “applicable plan” in 1862(b)(8)(F) which states that an applicable plan means liability insurance (including self-insurance), no-fault insurance, or a workers’ compensation law or plan;
- 3. amend §405.906 by adding §405.906(a)(4) to include the applicable plan as a party for the initial determination where Medicare is pursuing recovery directly from the applicable plan. By “pursuing recovery directly from the applicable plan,” CMS means that the applicable plan would be the identified debtor, with a recovery demand letter requiring repayment issued to the applicable plan (or its agent or representative). Sending an applicable plan a courtesy copy of a recovery demand letter issued to a beneficiary does not qualify as “pursuing recovery directly from the applicable plan” and does not confer party status on the applicable plan. The applicable plan’s party status would continue at subsequent levels of appeal (redetermination by the contractor issuing the recovery demand, a reconsideration by a Qualified Independent Contractor (QIC), an Administrative Law Judge (ALJ) hearing, a review by the Department Appeals Board’s (DAB) Medicare Appeals Council (MAC) and eventual judicial review). The beneficiary, provider, and/or supplier are not considered parties to an appeal by an applicable plan. Thus CMS proposes to remove the beneficiary, as well as the provider or supplier, as a party at the redetermination level where Medicare is pursuing recovery directly from the applicable plan. This would also, in effect, remove the beneficiary and the provider or supplier as a party at subsequent levels of appeal where Medicare is pursuing recovery directly from the applicable plan;
- 4. revise §405.906(a) to specify: (1) the circumstances under which an applicable plan is a party to an initial determination; and (2) when an applicable plan is a party to an initial determination, it is the sole party with respect to that determination. Since providers and suppliers would specifically be excluded from party status for an initial determination with respect to an applicable plan, CMS would make it clear that the special rule for provider or supplier party status in §405.906(c) does not apply to an initial determination with respect to an applicable plan;
- 5. in proposed §405.910 CMS would ad a new paragraph (e)(4) to provide the applicable plan with parallel rights to a beneficiary’s rights or a provider or supplier’s rights regarding the duration of an appointment of representation with respect to an MSP recovery claim;
- 6. revise §405.910(i)(4) so that the special provision that beneficiaries, as well as, their representatives must receive notices or requests in a MSP recovery case continues to apply only to beneficiaries. For all other parties, including an applicable plan, CMS would continue to follow the regulatory provisions in §405.910(i)(1) through (3);
- 7. add paragraph (c) to §405.921 to provide specific language regarding requirements for notice to an applicable plan. This language would parallel the existing language in that section of the regulations regarding the notice to beneficiaries;
- 8. add §405.924(b)(15) to provide that a determination that Medicare has a recovery claim where Medicare is pursuing recovery directly from an applicable plan is an initial determination with respect to the amount of or existence of the MSP recovery claim. This addition would generally parallel the existing provisions in §405.924(b)(14) addressing pursuing MSP recovery claims from a beneficiary, provider or supplier;
- 9. revising §405.926(k) by creating an exception to the broad rule in §405.926(k) to reflect the proposed addition of §405.924(b)(15) (where Medicare is pursuing recovery directly from an applicable plan);
- 10. adding §405.926(a)(3) to clarify that Medicare’s determination regarding who/what entity it will pursue with respect to an MSP recovery claim is not an initial determination for purposes of part 405 subpart I and is not subject to appeal;
- 11. add the word “facilitates” to the existing “sponsors or contributes to” language in §405.926(k) in recognition of CMS’ longstanding position that the concept of employer sponsorship or contribution has always included facilitation efforts;
- 12. add §405.927 to provide notice to the beneficiary of an applicable plan’s request for a redetermination to add language satisfying the requirement at section 1862(b)(2)(B)(viii) of the Act that the beneficiary receive notice of the applicable plan’s intent to appeal where Medicare is pursuing recovery directly from the applicable plan. As the beneficiary would not be a party to the appeal at the redetermination level or subsequent levels of appeal, we believe that a single notice at the redetermination level satisfies the intent of this provision. Also proposed is that the required notice be issued by the contractor adjudicating the redetermination request in order to ensure clarity and consistency in the wording of the notice.
Beginning April 28, 2015 CMS promulgated its final rule which now establishes an appeals process for Respondents’ contesting of conditional payments whereby “applicable plans” can now appeal (a) final conditional payment demands issued by Medicare if the applicable plan disputes the amount or liability owed and (b) where Medicare demands recovery of an overpayment.
Applicable plans include liability insurance (including self-insurance), no-fault insurance and workers’ compensation plans. With this final regulation in place insurance carriers now have the same appeal rights as claimants in workers’ compensation cases or plaintiffs in personal injury cases in the appeal of a conditional payment.
Under the regulation applicable plans will navigate a multilevel appeals process where recovery is pursued directly from the applicable plan, including:
- a. redetermination by the contractor issuing the recovery demand;
- b. reconsideration by a Qualified Independent Contractor;
- c. review by an administrative law judge;
- d. review by the Department of Appeals Board’s Medicare Appeals Council;
- e. federal judicial review
CMS hopes to resolve applicable plan appeals at the first two levels so appeals will not have to move on to the administrative law judge level.
The appeals process parallels the existing process for claims-based, fee-for-service claimant/plaintiff’s appeals as well as provider, physician, or other supplier appeals for both Medicare Secondary Payer and non-Medicare Secondary Payer situations.
Claimants or plaintiffs are not party to an applicable plan’s appeal at the redetermination level or subsequent levels of appeal. However, the claimant or plaintiff will receive notice that an applicable plan has submitted a request for appeal when an applicable plan requests a redetermination.
Section 202
This section of the Act provides in 42 U.S.C. §1395y(b)(2)(B)(ii)(9) commencing in 2014 the establishment an annual (not later than November 15th of each year) minimum liability single threshold (including alleged physical trauma-based incidents but excluding alleged ingestion, implantation, or exposure cases) for Section 111 reporting where the costs to CMS is greater than the recovery. This now creates an exception so that there will no longer by an obligation to repay Medicare under 42 U.S.C. 1395y(b)(2)(B)(ii) or to report under 42 U.S.C. 1395y(b)(8) if a qualifying claim falls below the annual calculated threshold. Author’s Comment: This threshold is suppose to reflect the average costs per claim CMS spends on recovery. I suspect it will be relatively low but the Act did not include a fixed threshold number. See Q & A 4 for a discussion of the MMSEA.
Section 203
This section of the Act allows under 42 U.S.C. 1395y(b)(2)(B)(8)(E)(1) a softening of Section 111 penalties giving CMS discretion when it issues such penalties. Now CMS may (as oppose to shall) impose a penalty of up to $1000 per day per claim rather than the current fixed $1000 penalty. Within 60 days of passage CMS must solicit public input for regulations addressing specification of practices for which sanctions will and will not be imposed.
In response on December 10, 2013 CMS published an Advance Notice of Proposed Rulemaking (ANPRM) regarding civil monetary penalties for failure to comply with the MSP. CMS solicited comments up to February 10, 2014 in three categories:
- a. practices for which penalties would or would not be imposed on reporting entities;
- b. methods to determine the dollar amounts of penalties to be imposed against a responsible reporting entity; and
- c. definitions and criteria to determine “good faith efforts” by workers’ compensation, liability and no-fault plans to identify Medicare beneficiaries for the purposes of reporting.
As of the date this Q & A was published no formal rules have been finalized.
Section 204
This section of the Act is effective eighteen (18) months after the passage of the Act which was on 1-10-13. 42 U.S.C. 1395y(b)(8)(B) makes the reporting of a beneficiary’s SSN and/or HICN optional for Section 111 reporting. See Section 5.02.1 of the text.
Section 205
This section of the Act is effective six (6) months after the passage of the Act and establishes under 42 U.S.C. §1395y(b)(2)(B)(iii) a 3 year statute of limitations on recovery efforts by CMS. The statute runs from 3 years after the date of the receipt via the MMSEA of notice of a settlement, judgment, award, or other payment.
Comment: On July 30, 2014 Congress sent a letter to CMS expressing its concerns that CMS has delayed implementing several aspects of the SMART Act raising concerns for entities responsible to comply with the statute and further delaying repayments of taxpayer dollars to the Medicare Trust Fund. Chief among these concerns was the delay to 2016 of the “expedited portal”, delay in establishing “thresholds” for liability claims which exempt those claims from the MSP recovery process; delays in establishment of “safe harbor” which protect stakeholders that make good faith efforts to comply with Medicare’s complex MSP reporting process under the MMSEA; and, delaying use of full Social Security numbers in the MMSEA reporting process.
A4. Comment: To the extent the Medicare, Medicaid and SCHIP Extension Act of 2007 or AMMSEA@ implicates itself in the settlement of workers’ compensation or liability claims it will be address. For a more comprehensive discussion of the MMSEA with CMS’ web site at: www.cms.gov/Medicare/Coordination-of-Benefits-and-Recovery/Mandatory-Insurer-Repo rting-For-Non-Group-Health-Plans/Overview.html
For the most current updates to the MMSEA or to review the various CMS transcripts discussing the MMSEA and its interrelationship with other provisions of the Medicare Secondary Payment Act the practitioners should visit www.cms.gov then click the Medicare tab then scroll down to the Coordination of Benefits & Recovery then scroll down to either the Mandatory Insurer Reporting For Group Health Plans (GRP) or Non Group Health Plans (NGRP) and from either site find NGRP or GRP transcripts
On December 29, 2007, former President George W. Bush signed into law the MMSEA which amended the Medicare Secondary Payer (MSP) provisions of the Social Security Act (Section 1862(b); 42 U.S.C. 1395y(b)) to provide for mandatory reporting for group health plan arrangements, liability insurance (including self-insurance), no-fault insurance, and workers’ compensation.
Comment: The MMSEA is an electronic claim reporting statute applicable to group health plans , third party administrators, fiduciaries of self-insured/self-administered group health plans, liability insurers (including self-insurers), no-fault insurers and workers= compensation insurers which targets insurance carriers and self-insured entities.
THE MMSEA DOES NOT REQUIRE USE OF MEDICARE SET-ASIDES IN EITHER WORKERS’ COMPENSATION OR LIABILITY CASES.
THE MMSEA IMPOSES NO REPORTING REQUIREMENTS UPON THE BENEFICIARY OR THEIR COUNSEL OR UPON DEFENSE COUNSEL. What the MMSEA does create is the concept of the “Responsible Reporting Entities” or “RRE” . These entities include all liability insurers, self-insurers, no fault insurers , group health insurers and workers’ compensation insurers. RREs are required to determine the Medicare eligibility status for the beneficiary and to report claim payments and settlements/judgments which involve a Medicare beneficiary.
The law is a mandatory insurer reporting law which requires certain entities to report information that Medicare requires for purposes of coordination of benefits between Medicare and other insurance and/or workers= compensation benefits. The primary purpose of this law is to verify any and all primary payers in incidents involving Medicare beneficiaries thereby assisting Medicare in its recovery efforts when it has paid benefits an otherwise primary payer should have paid.
THE MMSEA DOES NOT REPLACE THE REQUIREMENT THAT CLAIMS ALSO ARE REPORTABLE TO THE BENEFITS COORDINATION & RECOVERY CENTER. See Q & A
10. The MMSEA requires group health plan insurers, third party administrators, plan administrators, fiduciaries of self-insured/self-administered group health plans under 42 U.S.C. 1395y(b)(7), and liability insurers (including self-insurers), no-fault insurers and workers compensation insurers under 42 U.S.C. 1395y(b)(8), as directed by the Secretary of the Department of Health and Human Services, inter alia, to:
- a. determine whether a beneficiary is entitled to Medicare benefits on any basis (disability, retirement, survivor benefits etc…), and if so
- b. to report information that the Secretary requires for purposes of coordination of benefits between Medicare and other insurance and/or workers compensation benefits.
This mandatory claims data reporting has increased visibility into settlements where Medicare beneficiaries are involved and exposes all parties in the settlement to potential negative implications:
- a. the workers’ compensation carrier and/or employer may be exposed to double damages (1) if conditional payments are not reimbursed and CMS has to litigate to recover (42 U.S.C. §1395y(b)(2)(B)(iii));
- b. the beneficiary can bring a private cause of action for double damages against the workers’ compensation carrier or employer who fails to properly consider Medicare’s interests as part of the settlement (42 U.S.C. §1395y(b)(3)(A));
- c. if the beneficiary does not properly consider Medicare’s interests in the settlement of a workers’ compensation or liability claim the beneficiary may lose Medicare benefits for work or accident related medical services and prescription drug charges that would otherwise be payable or otherwise reimbursable by Medicare up to the full amount of the gross settlement proceeds;
- d. Attorneys may face potential malpractice claims for failure to protect the interests of their clients by proper investigation and reconciliation of various Medicare conditional payment claims and recovery claims made by Medicare Advantage Plans or Medicare Part D prescription drug plans.
In this respect the MMSEA identifies every settlement or judgment involving a Medicare beneficiary and therefore the practitioner must properly investigate and reconcile any conditional payments which are payable or otherwise reimbursable to Medicare as part of the settlement process and should commence this process well in advance of the settlement date or judgment.
Pursuant to 42 U.S.C. §1395y(b)(8)(E) failure to comply with these provisions will subject the carrier to a possible $1000 penalty for each day of noncompliance per beneficiary. Section 203 of the SMART Act allows under 42 U.S.C. 1395y(b)(2)(B)(8)(E)(1) a softening of Section 111 penalties giving CMS discretion when it issues such penalties. Under this provision CMS may (as oppose to shall) impose a penalty of up to $1000 per day per claim rather than the current fixed $1000 penalty. Within 60 days of passage CMS must solicit public input for regulations addressing specification of practices for which sanctions will and will not be imposed. The Act does not provide for a deadline when these proposed regulations are to be promulgated.
The MMSEA effective date for workers’ compensation and group health carrier’s reporting of claims is 1-1-09. The MMSEA effective date for liability and no-fault reporting of claims has been a moving target with varying reporting dates now extended between January 1, 2012 and January 1, 2013 depending on the total payment obligation or “TPOC”.
Comment: Section 202 of the SMART Act provides in 42 U.S.C. §1395y(b)(2)(B)(ii)(9) commencing in 2014 the establishment an annual (not later than November 15th of each year) minimum liability single threshold (including alleged physical trauma-based incidents but excluding alleged ingestion, implantation, or exposure cases) for Section 111 reporting where the costs to CMS is greater than the recovery. This now creates an exception so that there will no longer by an obligation to repay Medicare under 42 U.S.C. 1395y(b)(2)(B)(ii) or to report under 42 U.S.C. 1395y(b)(8) if a qualifying claim falls below the annual calculated threshold.
As of February 28, 2014 reporting thresholds for liability settlements, judgments, awards or other payments are as follows:
Mandatory Section 111 liability reporting thresholds for TPOCs are:
Settlements agreed to on or after 10-1-13 remains at amounts over $2000
Settlements agreed to on or after 10-1-14 moves to amounts over $1000
Minimum Section 111 reporting thresholds for TPOCs:
Settlements agreed to on or after 10-1-13 remains at amounts over $300
Settlements agreed to on or after 10-1-14 remains at amounts over $300
CMS did not increase the mandatory reporting thresholds for TPOCs related to workers’ compensation claims (mandatory reporting remains at amounts over $300). CMS has not set a minimum TPOC level for no-fault cases.
A5.Yes.First released on 3-1-2013 the Workers’ Compensation Medicare Set-Aside Arrangement (WCMSA) Reference Guide has been updated 6 times with the latest revision 2.3 being released on 1-5-2015. This guide was written by CMS to assist with the WCMSA CMS submission and approval process. The guide reflects information compiled from all previous CMS Regional Administrative Memorandums (see below), information provided on the various CMS websites, as well as, information from the WCRC and from CMS WCMSA Operating Rules. It should be considered the latest guidance from CMS in the submission and referral process and pre-exempts the previous CMS Regional Administrative Memorandums. It is expected this guide will be updated on a regular basis to keep the practitioner updated on CMS guidelines.
Beginning on July 23, 2001 and up to the release of the WCMSA Reference Guide CMS would issue various Regional Administrative Letters or “memorandums” explaining CMS’ policy and practice as it relates to the establishment, valuation and approval process for WCMSAs. These memorandums have been listed below. The vast majority of these deal exclusively with workers’ compensation claims. Memorandums Nos. 3, 17 and 18 deal with liability claims. The Stalcup handout (#17) and Release (#19) are not a Regional Administrative Letters but deal directly with liability claims.
A listing of the memorandums follows:
- Patel Memorandum dated July 23, 2001 entitled “Workers’ Compensation: Commutation of Future Benefits” (Parashar B. Patel, Deputy Director Purchasing Policy Group Center for Medicare Management)
- Olenick Memorandum dated October 15, 2001 entitled “Mr. Michael G. Dileo’s September 27, 2001 letter concerning Workers’ Compensation Cases” (Paul J. Olenick, Director, Division of Integrated Delivery Systems)
- Grissom Memorandum dated April 22, 2003 entitled “Medicare Secondary Payer Workers’ Compensation (WC) Frequently Asked Questions” (Thomas L. Grissom, Director Center for Medicare Management)
- Grissom Memorandum dated May 23, 2003 entitled “Medicare Secondary Payer Workers’ Compensation (WC) Additional Frequently Asked Questions” (Thomas L. Grissom, Director Center for Medicare Management)
- Herb Huhn Memorandum dated May 7, 2004 entitled “Medicare Secondary Payer- Workers’ Compensation (WC) INFORMATION” (Herb Kuhn, Director Center for Medicare Management)
- Walters Memorandum dated October 15, 2004 entitled “Medicare Secondary Payer (MSP)-Workers’ Compensation (WC) Additional Frequently Asked Questions”. (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated July 11, 2005 entitled “Medicare Secondary Payer (MSP)- Workers’ Compensation (WC) Additional Frequently Asked Questions” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated December 30, 2005 entitled “Part D and Workers’ Compensation Medicare Set-aside Arrangements (WCMSAs) Questions and Answers” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated April 25, 2006 entitled “Workers Compensation Medicare Set-Aside Arrangements (WCMSAs) and Revision of the Low Dollar Threshold for Medicare Beneficiaries” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated July 24, 2006 entitled “Questions and Answers for Part D and Workers’ Compensation Medicare Set-aside Arrangements” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated May 20, 2008 entitled “Medicare Secondary Payer – Workers’ Compensation – INFORMATION” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated August 25, 2008 entitled “Medicare Secondary Payer – Workers’ Compensation – INFORMATION” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated April 3, 2009 entitled “Medicare Secondary Payer – Workers’ Compensation – INFORMATION” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated May 14, 2010 entitled “Medicare Secondary Payer – Workers’ Compensation –INFORMATION” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Walters Memorandum dated June 8, 2010 entitled “Medicare Secondary Payer – Workers’ Compensation –INFORMATION” (Gerald Walters, Director Financial Services Group, Office of Financial Management)
- Benson Memorandum dated May 11, 2011 entitled “Medicare Secondary Payer – Workers’ Compensation – INFORMATION” (Charlotte Benson, Acting Director, Financial Services Group, Office of Financial Management)
- Stalcup handout dated May 25, 2011(Sally Stalcup, MSP Regional Coordinator, Division of Financial Management and Fee for Service Operations)
- Benson Memorandum dated September 29, 2011 entitled “Medicare Secondary Payer – Liability Insurance (Including Self-Insurance) Settlements, Judgments, Awards, or Other Payments and Future Medicals –INFORMATION” (Charlotte Benson, Acting Director, Financial Services Group, Office of Financial Management)
- “Liability Insurance (Including Self-Insurance): Exposure, Ingestion, and Implantation Issues and December 5, 1980 (12/5/1980)” dated October 11, 2011, Release by Office of Financial Management/Financial Services Group
- Benson Memorandum dated August 1, 2012 entitled “Impact of the Removal of coverage of Transcutaneous Electrical Nerve Stimulation (TENS) Units for Chronic Low Back Pain (CLBP) on Workers’ Compensation Medicare Set-Aside Arrangement (WCMSA) proposals – INFORMATION” (Charlotte Benson, Acting Director, Financial Services Group, Office of Financial Management)
- Tudor Memorandum dated October 2, 2012 entitled “Transition to Part D Coverage of Benzodiazepines and Barbiturates beginning in 2013” (Cynthia G. Tudor, Director, Medicare Drug Benefit and C & D Data Group)
Some of the original memorandums may be viewed by logging onto CMS’ web site: www.cms.gov/Medicare/Coordination-of-Benefits-and-Recovery/Workers- Compensation-Medicare-Set-Aside-Arrangements/WCMSA-Overview.html and clicking “Memorandums”.
In addition to these memorandums CMS has hosted open forum conference calls allowing practitioners to participate along with CMS management and staff in an informal “Q & A” format aimed at providing the practitioner with a better understanding of CMS’ requirements for the need to set up MSAs and the process by which that is accomplished.
A6. There are no statutory or regulatory provisions requiring that a WCMSA or LMSA amount be sought from CMS or that a WCMSA or LMSA be referred to CMS.
CMS codifies this in §§1.0 and 8.0 of the WCMSA Reference Guide when it states
“There are no statutory or regulatory provisions requiring that you submit a WCMSA amount proposal to CMS for review. If you choose to use CMS’ WCMSA review process, the Agency requests that you comply with CMS’ established policies and procedures”
Comment: Because the vast majority of existing regulations apply only to workers’ compensation claims there is great confusion as to whether or not there is any requirement for the use of the LMSA. Opponents of this view suggest (a) there is absolutely nothing in the statutes or regulations that mandate any personal injury settlement proceeds be “set-aside” for future medical services or prescription drug charges and (b) 42 U.S.C.§1395y(b)(2)(B)(ii) does not apply to post settlement/judgment medical expenses in liability cases. They argue that the reference to the term “reimburse” as found in 42 U.S.C. §1395y(b)(2)(B)(ii) makes it a subrogation statute for past or current payments and not to future payments. Those that advocate for this position suggest that once the case is closed, either by settlement or judgment, there is no longer a “primary” payer e.g., liability policy from which payment can be made or expected to be paid and therefore 42 U.S.C. §1395y(b)(2)(B)(ii) is not applicable. For a further discussion LMSAs see Q & A 37 & 38.
What the statutes and regulations do reinforce is that Medicare is statutorily secondary to any available primary payer policy, whether that policy is a workers’ compensation, liability or group health policy and that if a settlement “shifts” the primary payer status from a workers’ compensation, liability or group health carrier to Medicare and Medicare makes a “conditional payment” CMS has a priority right of recovery against any entity (beneficiary, provider, supplier physician, attorney, state agency or private insurer) that received a portion of the settlement proceeds either directly or indirectly. Medicare may also refuse to pay for future medical services or prescription drug charges related to the injury or illness until the entire settlement is exhausted. So proponents of the use of LMSAs in personal injury settlements recognize the existence of regulations and statutes since 1980 clearly provide that Medicare is a secondary payer to workers’ compensation, liability and group health policies and clearly provides Medicare the authority to deny payment when there is other valid and collectable coverage.
So exactly what are these statutes and regulations?
On 12-5-80 the Omnibus Budget Reconciliation Act of 1980 (94 Stat. 2599 , Pub L. No. 96- 499, §953; applicable regulations are found at 42 C.F.R. § 420 et seq.) enacted the Medicare Secondary Payer (MSP) Program codified in Section 1862(b)(A)(ii) of the Social Security Act (42 U.S.C. §1395y(b)(2)).
As discussed in Q & A 2 the essence of the MSP is to prevent the shifting of responsibility for payment of work or accident related medical services and prescription drug charges from a primary payer to Medicare.
42 U.S.C. §1395y(b)(2)(A)(I) and (ii) provides:
Payment under this subchapter may not be made, except as provided in subparagraph (B), with respect to any item or service to the extent that
(I) payment has been made, or can reasonably be expected to be made, with respect to the item or service as required under paragraph (1), or
(ii) payment has been made, or can reasonably be expected to be made under a workers’ compensation law or plan of the United States or a State or under an automobile or liability insurance policy or plan (including a self-insured plan) or under no fault.
42 U.S.C. §1395y(b)(2)(B)(ii) provides:
A primary plan, and an entity that receives payment from a primary plan, shall reimburse Medicare for any payment made by the United States under this subchapter with respect to an item or service if it is demonstrated that such primary plan has or had a responsibility to make payment with respect to such item or service. A primary plan’s responsibility for such payment may be demonstrated by a judgment, a payment conditioned upon the recipient’s compromise, waiver, or release (whether or not there is a determination or admission of liability) of payment for items or services included in a claim against the primary plan or the primary plan’s insured, or by other means.(emphasis added)
The MSP provides that Medicare may not make payment on behalf of a beneficiary for medical services or prescription drug charges where payment has been made or can reasonably be expected to be made promptly (42 U.S.C. §1395y(b)(2)(B)(I), 42 C.F.R. 411.21 (workers’ compensation), 42 C.F.R. 411.50 (liability), group health policy(42 U.S.C. §1395y(b)(2)(A)(ii), 42 C.F.R. 411.20(2).
Medicare regulations at 42 CFR 411.46 (workers’ compensation) states that:
“If a lump-sum compensation award stipulates that the amount paid is intended to compensate the individual for all future medical expenses required because of the work-related injury or disease, Medicare payments for such services are excluded until medical expenses related to the injury or disease equal the amount of the lump-sum payment.”
42 C.F.R. 411.46 therefore requires Medicare to exclude its payments when an individual receives a workers’ compensation settlement award that is intended to compensate the beneficiary for future medical expenses required because of a work-related injury or disease. That is, Medicare must not pay for an individual’s medical services or prescription drug when that individual received a workers’ compensation settlement, judgment or award that includes funds for future medical services or prescription drug charges, until all such funds are properly expended. Section 1862(b)(2) and 42 CFR 411.46 do not explicitly require individuals who are not yet Medicare beneficiaries to consult with CMS prior to settling their workers’ compensation cases. However, Section 1862(b)(2) and 42 CFR. 411.46 do require Medicare to exclude its payments once that eligible beneficiary actually becomes a Medicare entitled beneficiary.
Under the MSP Medicare has a priority right of recovery from the primary payer, as well as, from parties in receipt of third-party payments such as a beneficiary, provider, supplier, physician, attorney, state agency or private insurer (42 U.S.C. §1395y(b)(2)(B)(ii), 42 C.F.R. 411.25(g). This recovery can result in Medicare recovering the entire settlement amount to satisfy its recovery claim. In addition the Medicare manuals (§3407.8 of the MIM, §2370.8 of the MCM) state: “When a beneficiary accepts a lump-sum payment that represents a commutation [Q & A 25] of all future medical expenses and disability benefits, and the lump-sum amount is reasonable considering the future medical services that can be anticipated for the condition, Medicare does not pay for any items or services directly related to the injury or illness for which the commutation lump-sum is made, until the beneficiary presents medical bills related to the injury equal to the total amount of the lump-sum settlement allocated to medical treatment.”
In many situations, the parties to a workers’ compensation settlement choose to pursue a CMS approved WCMSA amount in order to establish certainty with respect to the amount that must be properly spent before Medicare begins to pay for claim related care. See, WCMSA Reference Guide, §2.3.
Comment: Accordingly, it is in the beneficiary’s best interest to “consider” Medicare’s interest well before the actual settlement date even though the beneficiary may not actually be a Medicare beneficiary at the time of settlement. Probably the most accepted method in which to document Medicare’s interests have been considered in a settlement is the utilization of either a WCMSA/LMSA. Remember this is an optional process and there could be alternative methods utilized to document the settlement “considers” Medicare’s interests. Beyond that, whether to utilize a MSA to protect the beneficiary’s future entitlement to Medicare coverage is totally independent of the resolution of the question as to whether the MSA is ever actually referred to CMS. See Q & A 51 for a discussion on CMS review thresholds.
Medicare Secondary Payer & Medicare Conditional Payments
Note: Medicare through the MSP and CRC will seek recovery from both group health plans (GHP) and non-group plans(NGHP). The discussion contained herein relates only to the NGHP plans.
A7. A “conditional payment” means Medicare made a payment for which another payer is claimed to be responsible. The payment is “conditional” because it must be repaid to Medicare when a settlement, judgment, award, or other payment is made.
Conditional payments are payments made for Medicare covered or reimbursable services or portions of services that are not paid under other coverage that is or was primary to Medicare and for which another payer is claimed to be responsible (42 C.F.R. 411.21(workers’ compensation), 42 C.F.R. 411.52 (liability claims)).
Medicare may make a “conditional payment” if an otherwise primary payer (liability, nofault, group insurance or workers’ compensation policy) does not pay or cannot be expected to be pay promptly (42 U.S.C. §1395y(b)(2)(B)(I), 42 C.F.R. 411.21, 42 C.F.R. 411.50). Promptly is generally defined to mean payment within 120 days after receipt of the claim. These conditional payments are made subject to being repaid to Medicare. A primary plan and any entity that receives payment from a primary plan shall reimburse Medicare for any payment made if it is demonstrated that such primary plan has or had a responsibility to make payment (42 U.S.C. §1395y(b)(2)(B)(ii)).
Medicare does not have a “lien” per se but rather has a statutory right of recovery for any “conditional payment” made due to the work or accident related injury or accident( 42 U.S.C. §1395y(d)(2)(b)).
Comment: The beneficiary always retains repayment obligations to Medicare and counsel for the beneficiary has the ethical obligation to inform the beneficiary of his or her repayment obligations including the possibility that failure by the beneficiary to reimburse Medicare for conditional payments may subject the beneficiary to collection action being brought against the beneficiary or interruption of beneficiary’s Social Security Disability or Medicare benefits if Medicare’s recovery claim is not paid. This should be documented in the practitioner’s file by use of an Informed Consent type document documenting client responsibility disclosure with counsel which memorializes the client’s understanding of his or her obligations and responsibilities.
A8. Whenever there is a pending liability, no-fault, or workers’ compensation claim, it must be reported to the BCRC. This is the first step in the MSP NGHP recovery process. All NGHP occurrences that involve a Medicare beneficiary should be reported to the Benefits Coordination & Recovery Center (BCRC). It is in the best interest of all sides to settlement discussions to have the most accurate information available regarding the amount owed to the BCRC.
The BCRC can be contacted by phone or mail to report a claim. BCRC Customer Service Representatives are available Monday through Friday, from 8:00 a.m. to 8:00 p.m., Eastern Time, except holidays. The BCRC’s toll free number is 1-855-798-2627 or TTY/TDD: 1-855-797-2627 for the hearing and speech impaired.
Written reports of WC occurrences should be addressed to:
Medicare—Medicare Secondary Payer
MSP Claims Investigation Project
P.O. Box 138899
Oklahoma City, OK 73113-8897
The practitioner will want to insure that the following information is available to initiate the process:
- a. Injured person’s name, address, telephone number, Social Security number(SSN) or Health Insurance Claim number(HICN), and date of birth
- b. Injured person’s attorney’s name, address and telephone number
- c. Employer (WC claims only) name and address.
- d. Insurer’s name, address, telephone number and claim number
- e. Insurer’s attorney’s name, address and telephone number
- f. Date of injury
- g. Body part(s)/system(s) related to the incident
- h. Related ICD-9/10 codes (preferred but not mandatory)
- I. Description of how injury occurred or illness was contracted
- j. Policy/claim number
See, WCMSA Reference Guide, § 2.2.
A9. Effective 7-1-12 CMS implemented a web based tool designed to assist in the resolution of workers’ compensation, liability and no-fault recovery cases. This tool is known as The Medicare Secondary Payer Recovery Portal or “WSPRP”.
The MSPRP User Guide was initially released on July 1, 2012 and has been updated 10 times through version 2.9 released on July 13, 2015.
Comment: the practitioner cannot initially request a file be opened through the MSPRP as this initial request to open the file must still be made to the BCRC either by telephone or mail as outlined in Q & A 8. Note that the current MSPRP is not the same web portal referenced in the SMART Act (See, Q & A 3).
In order to use the MSPRP the practitioner must:
a. first register at www.cob.coms.hhs.gov/MSPRP/. The registration process is relatively simple; however, the complete process will take approximately 30-45 days so that the CMS vetting process can be completed and
b. have the 15 digit “Case Identification Number” assigned by the BCRC.
The MSPRP provides the practitioner with the ability to access and update certain case specific information online. What use to require written correspondence or telephone calls to the MSPRC (predecessor to the BCRC) can now be done through the portal.
A10. The Coordination of Benefits & Recovery Center (COB&R) is responsible for protecting the Medicare program’s fiscal integrity and ensuring that it pays only for those services that are its responsibility. The COB&R has responsibility for both group health plan, whether self-insured or commercial (GHP) and non group health plan (NGHP) which includes workers’ compensation, automobile liability insurance, uninsured and underinsured motorist, no-fault insurance, personal injury protection, homeowner, liability insurance (including self-insurance), product liability and medical malpractice liability
Within the COB&R are two agencies: (a) the Benefits Coordination & Recovery Center or “BCRC” who has the responsibility for NGHP conditional payment reconciliation, and (b) the Commercial Repayment Center (CRC) who has responsibility for GHP conditional payment reconciliation. The BCRC was formerly two distinct entities e.g., the Coordination of Benefits Contractor or “COBC” and the Medicare Secondary Payer Recovery Contractor or “MSPRC”. This series of Q & As will address only NGHP issues.
The BCRC consolidates the activities that support the collection, management, and reporting of other insurance coverage for Medicare beneficiaries. The BCRC takes actions to identify the health benefits available to a Medicare beneficiary and coordinates the payment process to prevent mistaken payment of Medicare benefits. The BCRC does not process claims, nor does it handle any GHP related mistaken payment recoveries or claims specific inquiries. The Medicare Administrative Contractors (MACs), Intermediaries and Carriers are responsible for processing claims submitted for primary or secondary payment.
The BCRC can be contacted at the following mailing addresses:
Non-Group Health Plan (NGHP) Inquiries such as liability or no-fault insurance, automobile liability, uninsured or underinsured motorists, homeowners, malpractice, produce liability and general casualty insurance:
NGHP
P.O. Box 138832
Oklahoma City, OK 73113
31
Special Projects: (e.g. all Product Liability Case Inquiries)
Special Projects
P.O. Box 138868
Oklahoma City, OK 73113
BCRC Customer Service Representatives are available to assist you Monday through Friday, from 8:00 a.m. to 8:00 p.m., Eastern Time, except holidays, at toll-free lines: 1-855-798-2627 (TTY/TDD: 1-855-797-2627 for the hearing and speech impaired).The BCRC, regardless of claim type, may be contacted at 1-855-798-7627, 1-855-797-2627 (TTY/TTD), 1-405-869-3309(fax). As a general rule the caller will leave his or her name to schedule a call back time.
A11. Effective for cases established on or after October 1, 2009, the “Right to Recovery Letter” was issued by the COBC when a claim for liability insurance (including self-insurance), no-fault insurance, or workers’ compensation is reported to the COBC. As of July 2011 with the reorganization into the COB&R the letter is now issued by the BCRC. The letter was renamed the “Medicare Secondary Payer Rights and Responsibilities Letter”. The letter has been revised to omit the statement made in earlier letters that Medicare should be repaid before funds are disbursed for other purposes. It also adds a statement that Medicare will not take any collection action if an appeal or waiver request is pending.
Normally within 45 days of receipt of the initial BCRC acknowledgment letter the practitioner will be sent a “Medicare Secondary Payer Rights and Responsibility Letter” and brochure by the BCRC.
The Medicare Secondary Payer Rights and Responsibility Letter provides general information on Medicare’s and beneficiary’s respective rights, as well as, other parties responsibilities. The letter explains what happens after a Medicare beneficiary files an insurance or workers’ compensation claim, what information the BCRC needs, and what information the Medicare beneficiary can expect from the BCRC.
The beneficiary and any authorized individuals will receive a copy of this letter. It does not provide any conditional payment information. At this point the BCRC begins the process of assembling interim conditional payment information and will initiate recovery activities against the responsible party(s).
The attorney/representative will receive a copy of this communication and others from the BCRC as long as the attorney/representative has submitted a Proof of Representation (Q & A 16) or Consent to Release (Q & A 17). With one of these forms on file, the attorney/representative will also be sent a copy of the Conditional Payment Letter (CPL)(Q & A 12) and Final Demand Letter (Q & A 19). Note: In some special circumstances, the potential third party payer can submit a Proof of Representation giving the third party payer permission to enter into discussions with Medicare’s entities and which will allow them to receive CPLs and the Final Demand Letter.
This letter also provides the parties who have liability claims information about special options for resolving repayment of conditional payments including the (a) $1000 threshold, (b) fixed percentage option for repayment and (c) self calculating option. These options only apply to liability cases and are discussed in depth in Chapter 5 of the writer’s text entitled “Practitioner’s Reference Manual To Settlements, Offsets and Set-asides – Second Edition (see the introduction to this Q & A for information about the text).
The letter also contains the 15 digit “Case Identification Number” which will be necessary to have in order to access the MSPRP web portal, as well as, a Correspondence Cover Sheet with a specifically assigned bar code unique to the beneficiary’s file. Any written correspondence or information the practitioner submits to the MSPRC (other than what is inputted though the MSPRP) should utilize the cover sheet. For those practitioner
It is a good practice to diary the practitioner’s file for 10 days and then contact the BCRC by telephone to request the 15 digit case identification number. Once the practitioner receives this the proper authorization should be sent to the BCRC.
A12. Upon receipt of the notice of claim (Q & A 8) the BCRC begins identifying claims that Medicare has paid conditionally that are related to the case. Medicare’s recovery claim runs from the “date of incident” through the date of settlement/judgment/award (where an “incident” involves exposure to or ingestion of a substance over time, the date of incident is the date of first exposure/ingestion).
Once the BCRC has completed its initial investigation, but no later than 65 days after issuance of the Medicare Secondary Payer Rights and Responsibilities Letter (Q & A 11), the BCRC will provide either:
(a) the initial Conditional Payment Letter or “CPL” along with the Payment Summary Form or “PSF”. The conditional payment amount is considered an interim amount because Medicare may make additional payments while the claim is pending. If there is a significant delay between the initial notification to the BCRC and the settlement, judgment or award, the beneficiary/representative may request an interim CPL which lists the claims paid to date that are related to the no-fault, liability, or workers’ compensation claim. Comment: If the practitioner has register to utilize the MSPRP and has Multi-Factor Authentication (Q & A 9) there should be no need to request either the initial or interim CPL since it can be done through the portal.
Effective October 1, 2009, once the claim is open the BCRC will issue information concerning interim conditional payment amounts automatically (that is, without receiving a request for such information) as soon as an interim conditional payment amount is available. The CPL is accompanied by the Payment Summary Form (PSF).
The PSF will identify the total dollar amount to date of claims submitted to Medicare along with the total dollar amount to date constituting what the BCRC believes constitutes the Medicare conditional recovery amount. This is not a demand for payment and no payment is due at this time.
The scope of information contained in the PSF is contingent upon whether the practitioner obtained the PSF by requesting it through the mails or how the practitioner logs into the MSPRP portal. The information obtained through the mail, although slower to obtain, is as detailed as the information obtained by one who logs into the MSPRP with a Multi-Factor Authentication. The least specific information is obtained by a practitioner who logs into the MSPRP without using the Multi-Factor Authentication. The PSF is also available to the beneficiary via the MSPRP who does not have to log on using the Multi- Factor Authentication to obtained the more detailed PSF. Refer to Q & A 9 for a further discussion on the differences.
The PSF is also available to the beneficiary from www.mymedicare.gov and clicking the “MyMSP” tab. To use the MyMSP website it is necessary that the beneficiary register on the site and obtain a user password. This website will display information such as case type, conditional payments, total charges and the date the case was last updated but generally only does so for the last 18-24 months. The information from this website will be updated weekly with any changes or newly processed claims. Comment: “MyMSP” is not an official listing of Medicare claimed conditional payments but has quick and easy access for what can be best described as an estimated Medicare conditional payment claim. Its use does not constitute a substitution for reporting the claim to the BCRC and completing the Medicare conditional payment reporting process.
(b) send a confirmation letter along with a blank Final Detail Settlement Document (see Q & A 18) that no Medicare conditional payments have been made at the present time. Note that even if the BCRC issues a confirmation that no Medicare conditional payments have been made this will NOT be finalized until such time as the Final Detail Settlement Document is completed and returned to BCRC and in turn the practitioner receives from BCRC the Final Demand Letter (see Q & A 19).
The CPL also provides the beneficiary:
- a. a description of the responsibility the beneficiary has to Medicare regarding repayment.
- b. an explanation as to how to dispute any unrelated claims and includes the BCRC’s best estimate, as of the date the letter is issued, of the amount Medicare should be reimbursed (i.e., the interim total conditional payment amount).
The BCRC may issue one or more CPL/PSFs (depending on the number of Part A and Part B carriers the BCRC must contact). These PSFs will differ in amounts since Medicare may subsequently deny some claims or a beneficiary may incur additional medical services. These CPL/PSFs are advisoryonly and are subject to change as the MSPRC continues to investigate the conditional payments. The CPL is not a request for payment, rather the CPL/PSF provides a currently available itemized listing of Medicare conditional payments. Until the Final Demand Letter is issued one cannot, with any assurances, state that a final repayment obligation amount to BCRC has been determined.
It should also be pointed out that the PSF figures for reimbursed amounts and conditional payment amounts will differ from the amount a medical vendor may in fact have billed or what the medical vendor’s plan may” allow” or “reimburse” under its contract provisions.
Note that the BCRC does not include in the PSF Part C (Medicare Advantage Plans) or Part D (prescription drug) payments and does not seek recovery for either Part C or Part D payments made by a private insurance company. Keep in mind that private carriers administer Part C and D plan benefits and may allege a similar conditional payment lien. Comment: Presently there is a split in the Federal District courts as to whether these private carriers who are administering Medicare Part C or D plans have such a lien or right of recovery. For a further discussion the reader is directed to Chapter 5 of the writer’s text, “Practitioner’s Reference Manual to Settlements, Offsets and Set-asides – Second Edition” discussed in the introduction of this Q & A.
Once the CPLs are issued the practitioner can commence the reconciliation process of those items shown on the PSF.
This is an on-going process which, depending on the degree of dispute as to an entry(s) on the PSF may take a period of time to resolve. This process should start at least 6 months before the anticipated settlement date or trial.
Note: The for personal injury liability cases ONLY conditional payment amounts can also be obtained using the Fixed Percentage Option or the Self-Calculated Option. Under limited circumstances conditional payments of $1000 or less are not repayable to BCRC. For additional information related to the requirements of these programs visit https://www.cms.gov or the reader is directed to Chapter 5 of the writer’s text, “Practitioner’s Reference Manual to Settlements, Offsets and Set-asides – Second Edition” discussed in the introduction of this Q & A.
A13. What happens if BCRC receives notification via the MMSEA Section 111 reporting process that a settlement, judgment, award or other payment has already occurred?
If a settlement, judgment, award, or other payment has already occurred when the case is first reported, a conditional payment notice of “CPN” will be issued in lieu of a conditional payment letter (CPL). Like the CPL, the CPN provides conditional payment information and advises the beneficiary what action must be taken. The CPN is issued because the BCRC has been notified of a settlement, judgment, award or other payment thru the MMSEA Section 111 reporting process rather than from the beneficiary or beneficiary’s representative
The CPN allows for review of the conditional payment information in a similar vein as with the CPL. However, unlike a CPL, if there is a claim payment on the CPN not related to the case being reported normal dispute proceedings within a condensed time frame are to be followed.
The beneficiary or beneficiary’s counsel has 30 calendar days to respond. The following items must be forwarded to the BCRC if they have not previously been sent:
- a. Proof of Representation/Consent to Release documentation, if applicable;
- b. Proof of any items and/or services that are not related to the reported claim, if applicable
- c. All settlement documentation if the beneficiary is providing proof of any items and/or
services not related to the case;
- d. Itemization of any procurement costs and fees paid by the beneficiary
- e. Documentation of any additional or pending settlement, judgment, award or other payment related to the same incident
Note that like a CPL, conditional payments may increase after the issuance of a CPN if Medicare paid for additional items and or services related to the claim.
If a response is received within the 30 day window the BCRC will review it and issue a Final Demand Letter (see Q & A 19). If a response is not received within the 30 day window BCRC will issue a Final Demand Letter requesting repayment of all conditional payments related to the reported case without proportionate reduction for procurement fees or costs.
A14. Unless an update request for conditional payment information is received updated CPL amounts are generally unavailable until at least 90 days after the initial CPL is issued. CMS’ systems retrieve additional paid claims for each established case once every 90 days. The updated CPL information will appear automatically on the beneficiary’s “MyMSP” tab (Q & A 12) of the www.mymedicare.gov. website and is available from the MSPRP.
A15. If the beneficiary or beneficiary’s representative believes that any claims included on CPL/PSF or CPN/PSF should be removed from Medicare’s interim conditional payment amount, documentation supporting that position must be sent to the BCRC The BCRC will adjust the conditional payment amount to account for any claims it agrees are not related to what has been claimed/released.
The practitioner should allow 45 calendar days for the BCRC to review the submitted disputes and make a determination. During its review process, if the BCRC identifies additional payments that are related to the case, they will be included in a recalculated Conditional Payment Amount and updated CPL/CPN. If CMS determines that the documentation provided at the time of the dispute is not sufficient, the dispute will be denied. The beneficiary or beneficiary’s representative will receive a letter explaining Medicare’s determination once the review is complete.
See Q & A 8 & 9 for the process by which disputes are handled.
A16. This is the form wherein the beneficiary authorizes an individual or entity (including an attorney) to act on the beneficiary’s behalf in dealing with the BCRC. The representative has no independent standing, but may
- a. receive claims information from the BCRC
- b. respond to requests from the BCRC,
- c. provide necessary information to or interact with the BCRC in order to resolve Medicare’s recovery claim
- d. submit information/requests on behalf of the beneficiary to the BCRC
- e. receive a copy of the Final Demand Letter, and
- f. file an appeal with the BCRC (if appropriate).
Under these circumstances, the exchange of information is a two way street.
Along with the beneficiary’s signature the representative must sign and date the Proof of Representation authorization to confirm the representative has agreed to represent the beneficiary. If the Proof of Representation is not signed by the beneficiary then applicable court documents must also be submitted supporting that relationship e.g. guardian, conservator, power of attorney etc…. See, information Reference: WCMSA Reference Guide, §9.4.4, Step 1.
Comment: Should counsel for the beneficiary allow or refer resolution of Medicare conditional payments with another attorney or entity who has been provided a Proof of Representation then counsel should instruct the holder of the Proof of Representation to provide copies of all correspondence between the holder of the Proof of Representation and the BCRC so that the beneficiary’s attorney is kept abreast of the negotiations with the BCRC on the resolution of these conditional payments.
A sample Proof of Representation form follows:
Proof Of Representation
Type of Medicare Beneficiary Representative
(Check one below and then print the requested information)
Attorney other than an Attorney of record: Name: Angelo Paul Sevarino, Esq.
Address: 26 Barber Hill Road,
Broad Brook, CT 06016
Telephone: 860-716-0320
Attorney Relationship to the Medicare Beneficiary:
Guardian/Conservator Name: _____________________________
Address: _____________________________
Telephone: _____________________________
Power of Attorney Name: _____________________________
Address: _____________________________
Telephone: _____________________________
Medicare Beneficiary Information and Signature/Date:
Beneficiary’s Name (please print exactly as shown on the Medicare card):
______________________________________________
Beneficiary’s Health Insurance Claim Number (number on Medicare card): _____________________________
Date of Illness/Injury for which the beneficiary has filed a liability insurance, no-fault insurance or workers’ compensation claim: _____________________________
Beneficiary Signature: ___________________________ Date signed: ___________________
Representative’s Signature: _______________________ Date signed: ___________________
Angelo Paul Sevarino
A17. This is the form wherein the beneficiary has authorized an individual or entity to receive certain information from the BCRC or WCRC for a limited period of time. The release does not give the individual or entity the authority to act on behalf of the beneficiary.Under these circumstances, the exchange of information is a one-way street.
The beneficiary has authorized the CMS, including the BCRC/WCRC, to provide privacy protected data to the specified individual or entity, however this does not authorize the individual or entity requesting information to act on behalf of or make decisions on behalf of the beneficiary. If the Consent To Release is not signed by the beneficiary then applicable court documents must also be submitted supporting that relationship e.g. guardian, conservator, power of attorney etc…. WCMSA Reference Guide, §9.4.4, Step 1.
The Consent to Release authorization is the beneficiary’s signed authorization for CMS, its agents and/or contractors to discuss his or her case or medical condition with the parties identified on the authorization in regard to the workers’ compensation or personal injury settlement.
A sample Consent To Release Form is shown below:
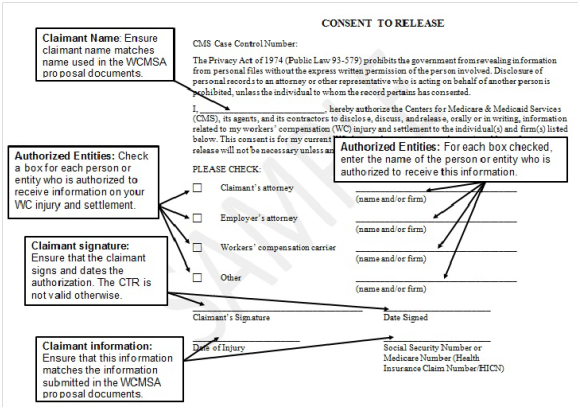
A18. Once the workers’ compensation or personal injury liability settlement has been finalized the “Final Settlement Detail Document” is prepared and sent to the BCRC or uploaded from the MSPRP. Note that for automobile no-fault claims the form is labeled “No Fault Case Closure Detail Document”.
A sample “Final Settlement Detail Document” and “No-fault Case Closure Detail Document” are shown below. It is a good practice to attach a copy of the settlement document or judgment to the Final Settlement or No-fault Case Detail Document.
Note, the practitioner does not submit payment of Medicare conditional payments at this time. Only after the settlement has been approved or a judgment entered and the Final Settlement or No-fault Case Detail Document is received by the BCRC will the BCRC finalize its recovery claim and issue its Final Demand Letter (Q & A 19). Only upon receipt of the Final Demand Letter can the practitioner know the actual final repayment amount claimed by the BCRC. The Final Demand Letter will indicate the amount of recoupment BCRC is seeking from the settlement, as well as, advising the beneficiary of rights to request a waiver or appeal.
Unless uploaded to the MSPRP the Final Settlement Detail Documents is sent to:
For Workers’ compensation, liability and no-fault, send to:
NGHP
PO Box 138832
Oklahoma City, OK 73113
Comment: This presents obvious problems for the practitioner since the settlement assumes Medicare conditional payments as advised by BCRC through the interim CPL/CPN. This means the practitioner must advise the beneficiary that the practitioner will not be able to guarantee what the actual final Medicare conditional payment recovery amount will be at the time of settlement. Should the practitioner later be advised that the conditional payments are more than previously reported the practitioner may be personally liable for the difference should the beneficiary not have funds available. It is therefore recommended that full settlement proceeds not be disbursement until after the Final Demand Letter has been received, any disputes filed with the BCRC concluded and the practitioner has received a release from the BCRC indicating all claims for recovery have been reconciled. Assuming the practitioner has completed a bona fide good faith effort to identify those PSF entries that are related to the work or accident date of injury it is suggested that the practitioner retain in the practitioner’s IOLTA or client’s fund at least an additional 25% of the amount indicted in the Final Settlement Detail Document until the Final Demand Letter is received from BCRC.
Sample Final Settlement Detail Documents are shown below:
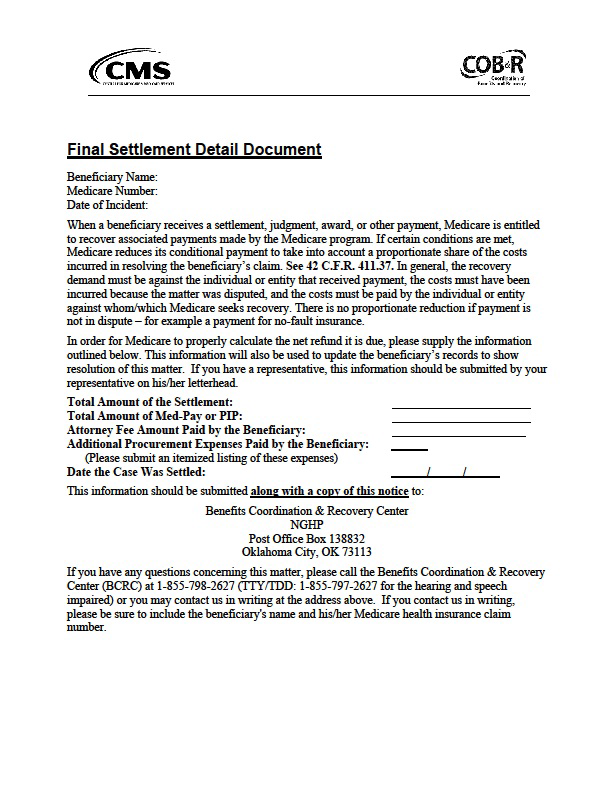
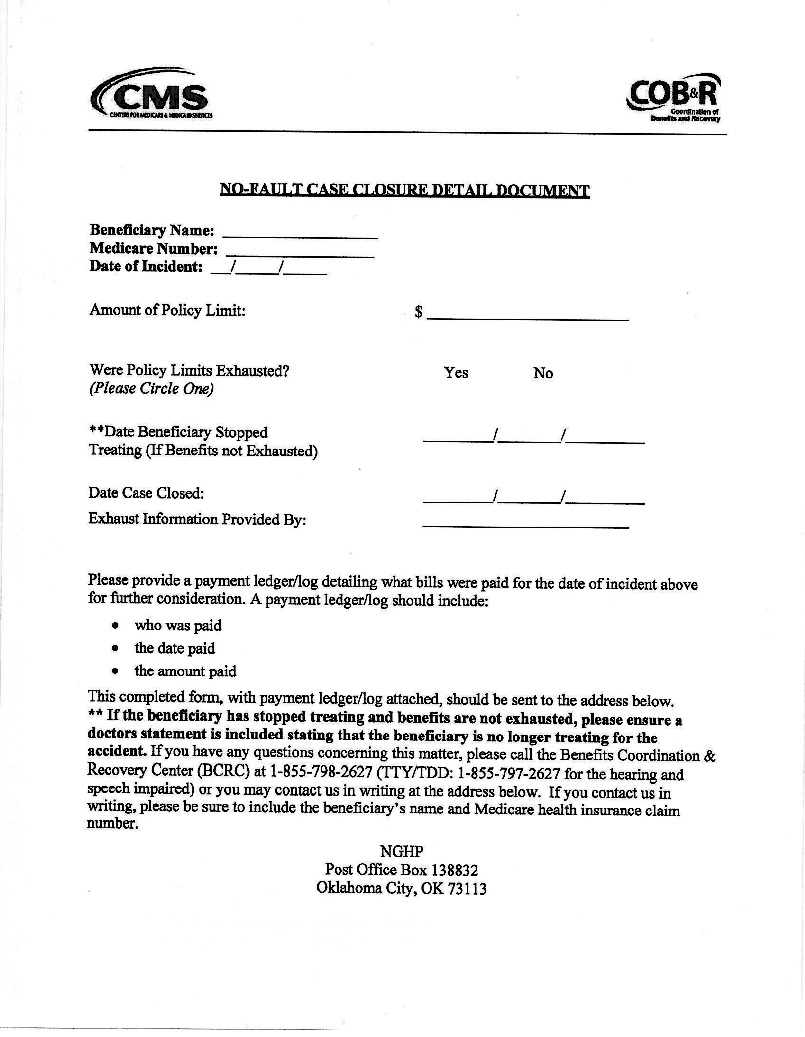
A19. Upon receipt of the Final Settlement Detail Document (Q & A 18) the BCRC will either send the practitioner a “Final Demand Letter” or a letter indicating no conditional payments were made and their file is closed. As a general rule the BCRC has 35 days to issue the Final Demand Letter. If the practitioner should not receive this letter within the 35 day period the practitioner should call the BCRC and inquire.
The BCRC will apply a termination date (generally the date of settlement, judgment, award, or other payment) to the case. The BCRC will identify any new, related claims that have been paid since the last time the CPL/CPN was issued up to and including the settlement, judgment or award date. Once this process is complete, the BCRC will issue a formal Final Demand Letter advising the debtor (Medicare beneficiary or insurer) of the amount of money owed to the Medicare program. The amount of money owed is called the Demand Amount.
The Final Demand Letter includes the following information:
- a. the beneficiary’s name and Medicare Health Insurance Claim Number (HICN)
- b. date of accident/incident
- c. a summary of conditional payments made by Medicare
- d. the total Demand Amount, and
- e. information on applicable waiver and administrative appeal rights
The Final Demand Letter will also indicate a notice that payment is due within 60 days, and provide notice of penalties and interest of 11% will accrue if payment is delayed, as well as, collection efforts and appeal or waiver options. The BCRC will also advise the beneficiary that should the Medicare recoupment claim not be paid and, if the beneficiary is receiving Social Security disability benefits, that it will be deducted from the beneficiary’s Social Security monthly check.
A20. Yes. Medicare’s reimbursement claim against the beneficiary can be reduced by a formula that recognizes the pro-rata share of procurement costs e.g., attorney fees and most costs associated with the prosecution of the claim.
A21. No. Medicare cannot make a formal determination until the beneficiary actually becomes entitled to Medicare. However, once the beneficiary becomes Medicare entitled, Medicare payment may not be made to the extent of Medicare’s interests in the lump sum payment (42 CFR 411.46) or according to any WCMSA to be established that adequately consider Medicare’s interests.
A22. Neither. Medicare should not pay these bills because it is secondary to the workers’ compensation or liability settlement. The WCMSA cannot pay these bills because it is created solely for future medical and prescription drug expenses related to the case.
Medical expenses incurred prior to the settlement need to be accounted for and paid from the settlement proceeds, exclusive of any sums allocated to a WCMSA. These medical services and prescription drug charges should have been documented by the parties in advance of the settlement. The provider/supplier may have billed Medicare, a group health carrier or the workers’ compensation carrier for these medical services or prescription drug charges and the beneficiary’s representative should have made inquiries about outstanding related bills. To the extent Medicare has paid these bills, and therefore made conditional payments, Medicare will recover those payments pursuant to 42 C.F.R. 411.47. See, WCMSA Reference Guide §4.1.2.
A23. Under 42 U.S.C. 1395y(b)(2)(A) and certain regulations found at 42 C.F.R. §§411.22 – 411. the MSP prohibits Medicare from making payments if payment has been made or is reasonably expected to be made by a workers’ compensation plan, liability insurance, no-fault insurance, or a group health plan. This same statute and regulations require that a primary payer and any entity (defined as the beneficiary, provider, supplier, physician, attorney, State agency or private insurer) that receives payment from a primary payer is required to reimburse Medicare if it is demonstrated that such primary payer has or had responsibility to make the payment initially.
CMS therefore has a direct priority right of recovery against any entity including a beneficiary, provider, supplier, physician, attorney, state agency, or private insurer that has paid or received any portion of the settlement proceeds whether directly or indirectly. CMS also has a subrogation right with respect to any such third party payment. See, for example, 42 C.F.R. 411.24(b), (e), and (g) and 42 C.F.R. 411.26.
This means that Medicare’s right of recovery for past medical services and prescription drug charges which were made extends to all those medical services and prescription drug charges related to what was claimed and/or released in the settlement, judgment or award. The term “past medical services” refers to Medicare payable or otherwise reimbursable items and services that the beneficiary receives before s/he obtains a workers’ compensation settlement, judgment, award or other payment. See, WCMSA Reference Guide, §2.3.
Medicare’s payment for those past services and charges are therefore recoverable and payment for those services and charges is precluded by 42 U.S.C. §1395y(b)(2)(B)(ii).
Comment: This right of recovery clearly applies to any conditional Medicare payments made prior to the settlement; however there is no clarity as to whether CMS has a direct right of recovery under 42 U.S.C. §1395y(b)(2)(B)(ii) against any entity for payments Medicare may make for services provided after the settlement. Proposed legislation addressing this issue has not been passed and is needed to provide clarity and finality to the question.
Workers’ Compensation Medicare Set-asides (WCMSA)
A24. A Life Care Plan is a dynamic document based on published standards of practice, comprehensive assessment, data analysis, and research that provides an organized concise plan for current and future needs (both medical and otherwise) with associated costs for individuals who have experienced catastrophic injury or have chronic health needs. A life care plan is appropriate when the individual’s injury or disease is extensive and serious, e.g., paraplegia, quadriplegia, brain damage. A Life Care Plan is calculated based upon actual charges and will include both Medicare covered and non-Medicare covered medical services and prescription drug charges related to the injury or illness. It will also cover accident or work-related expenses other than medical services and prescription drug charges. As a general rule it is much more comprehensive than a Medicare Setaside analysis.
On the other hand a MSA is narrower in scope and less comprehensive than a Life Care Plan. For a more detailed explanation of what a MSA is the reader should review Q & A 25.
Both the Life Care Plan and MSA include pricing charts, cost projections, pricing information, specific medical services and items, pharmacy drug name, frequency and dosage and explanatory narratives and analyses. Such a Life Care Plan or MSA evaluation is not automatically conclusive. CMS may not credit the report if there is information that calls the evaluation or plan into question for some reason, such as contrary evidence, internal conflicts, or if the plan is not credible on its face.
If so instructed the preparer of a Life Care Plan can also provide the necessary data and calculations to identify those Medicare payable or otherwise reimbursable medical services and items and prescription drug charges which would be included in the MSA analysis.
See, WCMSA Reference Guide, §10.4.
A25. CMS defines a MSA as an administrative mechanism used to allocate a portion of a settlement, judgment or award for future medical services or items and/or future prescription drug expenses (CMS MSP Manual, Rev. 65, 03-20-09 at §20). CMS will rely on medical records and reports prepared by the beneficiary’s treating physician. If the MSA is based upon non-treating physician’s records and reports. While CMS will consider these non-treating physician’s records and reports it is free to disregard those evaluations.
A WCMSA allocates a portion of the workers’ compensation settlement for all future claim related medical services and prescription drug costs that are payable or otherwise reimbursable by Medicare (“Medicare covered”). When a proposed WCMSA amount is submitted to CMS for review and the claimant (who may or may not be a Medicare beneficiary) obtains CMS’ approval, the CMS approved WCMSA amount must be properly spent before Medicare will begin to pay for medical or prescription care related to the workers’ compensation claim.
A comprehensive MSA will include:
- a. Claimant demographics
- b. Claimant Medicare entitlement Information
- c. Injury or accident information, including description and occurrence information
- d. date(s) of injury/illness
- e. related body part(s)/system(s) included in the MSA
- f. related ICD9/10 diagnosis codes
- g. settlement details
- h. total proposed MSA amount
- I. MSA medical services amount including method of calculation
- j. MSA prescription drug therapy amount
- k. MSA Funding (lump sum or structured with seed/feed amounts)
- l. MSA administration (self-administered or professional)
- m. medical records review summary
- n. unrelated medical conditions not included in the MSA
- o. related medical care summary
- p. current medical treatment and prognosis
- q. projected medical treatment plan including CPT code, frequency & duration of need, unit cost, yearly units, annual costs, life expectancy duration, and
- r. total cost over life of beneficiary by physician/health care provider, surgeries, therapy, diagnostic testing, durable medical equipment and prescription drug therapy
The goal of establishing a WCMSA is to estimate, as accurately as possible, the total cost that will be incurred for all medical service and prescription expenses that are payable or otherwise reimbursable by Medicare for claim related conditions during the course of the beneficiary’s life, and to “set aside” sufficient funds from the settlement, judgment, or award to cover that cost.
WCMSAs may be funded by a lump-sum single payment, or may be structured, with a fixed amount of funds paid each year for the beneficiary’s life expectancy unless the state’s workers’ compensation statute allows for a shorter period of time.
If Medicare’s interests are not considered, CMS has a priority right of recovery against any entity that received any portion of a third party payment either directly or indirectly—a right to recover, or take back, that payment. CMS also has a subrogation right with respect to any such third party payment.
The WCMSA is typically not created until the beneficiary’s medical condition has stabilized, so that it can be determined based on past experience what the future medical expenses may be. CMS prefers this, so that future medical and prescription drug costs can be planned with a reasonable degree of certainty.
Once the CMS approved MSA amount is properly depleted and accurately accounted for to CMS, Medicare will pay primary for future Medicare payable or otherwise reimbursable medical services and prescription drug expenses related to the workers’ compensation claim that exceed the approved WCMSA set-aside amount.
See, WCMSA Reference Guide §3.0
A26. No. CMS has no process to accept up-front cash payments in lieu of a CMS reviewed WCMSA. See, WCMSA Reference Guide, §15.2.1.
Comment: : Over the years federal legislation has been proposed that would allow prepayment of a flat percentage of the gross settlement directly to Medicare to act as a “safe harbor” in lieu of doing a traditional WCMSA, however, passage of such legislation has been elusive. For a further discussion on legislative action the reader is referred to my text Practitioner’s Reference Manual To Settlements, Offsets & Set-asides – Second Edition published by Atlantic Law Book Company, West Ha r t fo rd , Co n ne c t i c u t 0 6 1 1 0 Th e r e a d e r i s en c o u r a ge d t o v i s i t : www.atlanticlawbooks.com/practionersGuide.htm.
A27. A settlement is an executed settlement agreement that is approved by the court or agency of competent jurisdiction for the applicable state and will be recognized by Medicare. Medicare is not required to recognize a settlement that has not been approved by the appropriate court or agency.
A28. Medicare’s regulations 42 C.F.R. 411.46 and manuals MIM 3407.7 & 3407.8 and MCM 2370.7 & 2370.8 make a distinction between settlements that are commutations of future benefits and those that are due to a compromise of past benefits between the insurance carrier and the beneficiary.
Compromise cases are settlement awards for a beneficiary’s current or past but not future medical services or prescription drug expenses (expenses incurred prior to the settlement date) that were incurred because of a work or accident injury or illness.
When a settlement includes compensation for future medical and/or prescription expenses, it is referred to as a “commutation case.”Commutation cases are settlement awards intended to compensate individuals for future medical services or prescription drug expenses (expenses incurred after the settlement date) which are required because of a work or accident related injury or disease. A settlement also has a commutation aspect if it does not provide for future medical expenses when the facts of the case indicate the need for continued medical care or prescription drug charges related to the workers’ compensation claim. See, WCMSA Reference Guide, §4.1.1.
When a settlement includes compensation for future medical and/or prescription expenses, It is important to note that a settlement agreement can possess both compromise and commutation aspects. That is, some settlement agreements can designate part of a settlement for a beneficiary’s future medical services or prescription drug expenses and simultaneously designate another part of the settlement for all of the beneficiary’s medical or prescription drug expenses up to the date of settlement.
A29. Accordingly to CMS, if in its opinion the settlement does not adequately consider Medicare’s interests it is not bound by the agreement. See Q & A 96 regarding a “hearing on the merits”.
A30. A settlement that does not specifically account for past versus future medical or prescription drug expenses will be considered to be entirely for future medical or prescription drug expenses (once Medicare has recovered any conditional payments it may have made). This means that Medicare will not pay for medical or prescription drug expenses that are payable or otherwise reimbursable under Medicare and are related to the workers’ compensation or personal injury occurrence until the entire settlement is exhausted.
Example: A beneficiary is paid $50,000 by an insurance carrier, and the parties to the settlement do not specify what the $50,000 is intended to pay for. Medicare has made $5,000 in conditional payments. If there is no allocation stated in the settlement agreement Medicare will consider $45,000 as compensation for future medical and prescription expenses.
A31. No. There is no means by which a beneficiary can permanently waive his or her right to certain specific services related to a workers’ compensation or liability case and, thereby, reduce the amount of a WCMSA/LMSA. CMS cannot approve settlements that promise not to bill Medicare for certain services in lieu of including those services in a WCMSA (the same logic would apply to an LMSA had a review by CMS been allowed). This is true even if the beneficiary offers to execute an affidavit or other legal document promising that Medicare will not be billed for certain services if those services are not included in the MSA. See, WCMSA Reference Guide, §15.2.2.
A32. No. A WCMSA would be unnecessary if the medical portion of the workers’ compensation claim remained open and the workers’ compensation carrier continues to be responsible for work related medical services or prescription drug costs since the workers’ compensation carrier remains the primary payer and Medicare retains its secondary payer status. See, WCMSA Reference Guide, §4.2.
A33Yes. Parties to the settlement may settle the indemnity (non medical expenses) portion of the claim separately from the WCMSA portion, in order to avoid having indemnity payments continue while CMS is still reviewing the proposal. Should the medical component of the claim later be settled CMS will still consider the whole claim, including indemnity and medical components, in its determination of whether referral the applicable threshold has been reached.
A34. Yes, a WCMSA is still appropriate because such other collateral health insurance or health service could in the future be canceled or reduced, or the beneficiary may elect not to take advantage of such medical services or prescription drug coverage. It is important to remember that workers’ compensation, liability or group health coverage is always primary to Medicare for expenses related to the workers’ compensation (or liability) settlement. See, WCMSA Reference Guide, §4.1.3.
A35. MSAs are not subject to any special treatment under Medicaid resource rules. The WCMSA funds should be evaluated to determine if they meet the legal definition of a resource for Supplemental Security Income (SSI), and therefore Medicaid, purposes, i.e., “cash or other assets that an individual owns and could convert to cash to be used for his or her support and maintenance.”
There may be cases in which funds in a MSA are placed into trusts, possibly trusts that would satisfy the definition of “special needs trusts” under Section 1917 of the Social Security Act. In those cases, the funds might not be a countable resource, but that result would be solely on the basis of Medicaid, not Medicare, rules. Consultation with an Elder Law specialist should be sought.
A36. The simple answer is that it will reduce the financial payout Medicare would otherwise have made and therefore remove some of the financial strain placed on the Medicare system. According to CMS, because a MSA’s purpose is to pay for all medical services and prescription drug charges related to the beneficiary’s work or accident related injury or illness, Medicare will not make any payments (as a primary, secondary or tertiary payer) or pay portions of medical services or prescription drug expenses for any medical or prescription drug charges due to the work or accident related injury or illness until no further funds remain in the MSA.
Comment: : The obvious bureaucracy created by the entire CMS referral process and the associated costs are not readily available for public scrutiny. The genesis of the CMS referral process was to save Medicare funding by insuring primary payers paid when appropriate. This is an admirable purpose and supported by all those injured workers and accident victims who are put in harm’s way. However, the costs of this CMS referral process must be in the forefront of any political arena that wishes to engage in the debate on Medicare funding as an entitlement. Only then will the true costs of Medicare program be out there for all to see.
Liability Medicare Set-asides (LMSA)
A37. No, however, some CMS Regional Offices are reviewing voluntarily submitted LMSA proposals. Comment: : Until such time as CMS promulgates review thresholds for LMSAs the referral of a proposed liability settlement to CMS would suggest an unnecessary exercise given CMS’ current absence of any due process appeal rights to their analysis.
Effective 9-29-11 CMS announced its first “guideline” specifically addressing the LMSA (Benson Memorandum dated September 29, 2011 entitled “Medicare Secondary Payer – Liability Insurance (Including Self-Insurance) Settlements, Judgments, Awards, or Other Payments and Future Medicals –INFORMATION” (Charlotte Benson, Acting Director, Financial Services Group, Office of Financial Management)). In this memorandum CMS considered its interest in a personal injury case satisfied if the treating physician “certifies in writing” that the treatment for the alleged injury related to the liability insurance (including self-insurance) settlement has been completed as of the date of the “settlement”, and that future medical items and/or services for that injury will not be required. If the plaintiff receives additional settlements (e.g., UM/UIM) related to the underlying injury or illness the plaintiff must obtain a separate physician certification for those additional settlements. When the treating physician makes such a certification, there is no need for the plaintiff to submit the certification or a proposed LMSA amount for CMS review.
As with workers’ compensation cases CMS will not provide the settling parties with confirmation (known as verification letters) that Medicare’s interest with respect to future medicals for that settlement has been satisfied. CMS suggests the certification be maintained in the file. See, WCMSA Reference Guide, §§4.2, 8.1.
Comment: : What constitutes a “certification” is not defined by CMS. Is it sufficient that the treating physician states his or her opinion within a reasonable degree of medical probability? Does the “certification” have to be acknowledged? Physicians are most likely to resist signing an affidavit entitled “certification” for fear that the document may someday surface in a malpractice action. Careful drafting of the settlement documents is warranted and in the case of a court side judgment the transcript should reflect no future medical costs have been awarded and in the case of jury verdicts special interrogatories to the jury should be submitted to confirm no award for future medical costs.
As with workers’ compensation settlements there is no statutory or regulatory authority for CMS’ position to utilize the LMSA process other than the Regional Director Memorandums interpreting the statutes and regulations. Reference may be had to The Centers for Medicare and Medicaid Services, NGHP Transcript, Town Hall Teleconferences: October 29, 2008 at page 18; September 30, 2009 at page 25; October 22, 2009 at page 64 and March 2010 at page 41 both indicating a lack of statutory or regulatory requirement for the use of or referral of a LMSA and that the referral process is entirely optional.
Comment: It is unrealistic to attempt to distinguish a liability only settlement as somehow exempt from §1826(b)(2)(A)(ii) which clearly mandates that Medicare is a secondary payer to liability and no-fault coverage. This law has been in effect since 12-5-1980 but only due to the fiscal crisis Medicare finds itself has CMS’ aggressive stance been seen. Make no mistake about it if there is a future medical component in a liability settlement or judgment Medicare will expect that amount to be exhausted before it steps up to the plate to pay. If there is no allocation whatsoever (e.g. simply a general release) expect Medicare to take the position that it does not have to pay for accident related medical services and prescription drug charges until the full amount of the settlement or judgment has been exhausted. Taking a proactive approach by utilization of a LMSA will go a long way to protect a client’s continued or potential entitlement to Medicare coverage once the LMSA is properly depleted and alleviate the client having to undergo the long arduous process of appealing a Medicare payment denial to the ALJ.
A38. Yes. This situation is commonly referred to as a “moratorium” or “credit” where the workers’compensation carrier’s liability for future medical services or prescription charges is stayed until the moratorium or credit amount is depleted. To the extent that a liability settlement is made that relieves a workers’ compensation carrier from any future medical expenses then CMS suggests either a WCMSA or LMSA be utilized (but not both).
Tax Implications with use of MSA
A39..26 U.S.C. §§ 104(a)(1), 104(a)(2) exclude from the definition of “gross income”
- a. compensation received for personal injuries or sickness except for punitive damages or
- b. workers’ compensation payments which are paid in lump sum or as periodic payments
This would allow the beneficiary the right to exclude lump sum or structured funding of the MSA(26 U.S.C. §130) from the taxable gross income of the beneficiary’s Social Security number used to establish the MSA.
With lump sum funded MSAs any interest generated by the MSA will also generate an INT- 1099 which is reportable on the beneficiary’s annual tax return. Assuming there is adequate documentation for the amount of incremental tax that the beneficiary must pay for the interest earned on the MSA funds, the beneficiary or his/her administrator may withdraw an amount equal to the incremental tax as a cost that is directly related to the MSA account to cover the additional tax liability.
Documentation of any such incurred interest and incremental tax liability should be submitted to CMS along with the annual accounting.
Administration of the MSA
A40.MSAs may be administered by:
- a. a competent beneficiary (self-administered), if State law allows
- b. a representative payee for Social Security purposes pursuant to 20 C.F.R. 404.2010 and 404.2015 such as a spouse or adult child (e.g., an individual appointed by the SSA to receive Social Security and/or SSI benefits for someone who cannot mange or direct someone else to manage his or her money because the individual is legally incompetent, mentally incapable of managing benefit payments, etc.)
- c. an appointed guardian or conservator (where the MSA is administered by a conservator or guardian oversight of the MSA by Probate court or court of competent jurisdiction will most likely be required)
- d. special needs trust, or
- e. a professional administrator
Administrators who fall within b-e above must provide CMS supporting documentation including the name, address, telephone and fax numbers of the administrator establishing their administrative capacity on behalf of the beneficiary. See, WCMSA Reference Guide, §§10.6, 17.1.
Administration of a MSA by other than a professional administrator knowledgeable in CMS rules and guidelines e.g., self-administration by the beneficiary is the most risky administration type since most beneficiaries (or their spouse, guardian, conservator or representative payee) have little if any:
- a. knowledge of Medicare coverage provisions that allow the administrator the ability to identify what “payable or otherwise reimbursable by Medicare” means
- b. experience with state medical fee schedules
- c. understanding of what Medicare deductibles, co-pays and coinsurance provisions are and how they are applied
- d. ability to negotiate fees submitted by medical vendors to conform with the terms of the MSA, and
- e. formal education necessary to properly account for the disbursement of MSA funds.
Use of a self-administered MSA should only be had after discussion with the client as to his or her abilities to comply with the process. If there is any doubt as to the designated administrator’s ability to properly administer the MSA and, if professional administration is not elected, self-help vendors are available by investigating the internet. Fees vary but normally range annually from $375 to $2000 depending on the period of time the administrator needs assistance, the scope of services requested and the dollar amount of the MSA.
A41.. All administrators of a MSA regardless of designation are required to follow the same rules, guidelines and reporting requirements. See, WCMSA Reference Guide, §17.1.
It is the administrator’s responsibility to:
- a. establish the MSA account in a FDIC insured bank or NCUSIF protected credit union
- b. disburse only Medicare covered or otherwise reimbursable expenses for medical services and prescription drug charges related to the settled accident or work related injury according to the terms of the MSA
- c. inform the various medical service providers or the pharmacy(s) that the MSA has been established
- d. advise the medical service provider(s) and pharmacy(s) not to bill Medicare or other credible health insurance that should not be primary to the MSA for any work or accident related charges
- e. advise the medical service provider as to the fee (state fee schedule or full actual charges) that may be payable from the MSA and to have this fee accepted for payment. If necessary the administrator must negotiate with the medical service provider(s) to accept payment according to the state fee schedule established in the MSA unless the MSA has been calculated based upon full actual charges
- f. when the MSA is structured the administrator must advise (should the annual amount available in the MSA be depleted) the medical vendor or pharmacy to again start billing Medicare (at current Medicare rates), advise the beneficiary, medical vendor or pharmacy as to when the MSA again becomes primary and therefore again to stop billing Medicare
- g. perform the annual accounting
Every year, beginning no later than 30 days after the 1 year anniversary of the establishment of the MSA or the 1 year anniversary of settlement of the workers’ compensation or personal injury claim, whichever is earlier, the administrator must sign and send an annual attestation accounting statement identifying each payment from the MSA which was made for Medicare payable or otherwise reimbursable medical services or covered prescription drugs related to the workers’ compensation or liability settlement. The annual accounting continues through proper depletion of the MSA funds or upon the death of the beneficiary.
See, WCMSA Reference Guide, § 6.0, §17.5.
A42. Initially CMS answered this question in the affirmative if all of the following were found to be true: the fee or costs were related only to the MSA itself; the fee or costs were reasonable in amount, and the fee or costs were included in the proposed MSA amount submitted to CMS and incorporated into the MSA approved by CMS.
However, as of May 7, 2004 administrative fees for the administration of the MSA and/or attorney fees and costs specifically associated with establishing the MSA cannot be included in the MSA amount, charged to or paid from the MSA. CMS no longer evaluates the reasonableness of any of these fees or costs because (a) CMS considers those a separate issue for the settling parties to negotiate and (b) the payment of these fees and costs must come from some other payment source that is completely separate from the MSA funds. See, WCMSA Reference Guide, §15.2.1.
While neither administrator fees for services rendered to administer the MSA nor attorney costs for establishing the MSA be charged to or paid from the MSA certain administrative “costs” that are directly related to the administration of the MSA are allowed to be paid from the MSA.
The administrator may use the MSA account to pay for the following costs that are directly related to the MSA account:
- a. document copying charges
- b. mailing fees/postage
- c. any banking fees related to the account
- d. income tax on interest income from the set-aside account (see, Q & A 39)
CMS Review Criteria and Procedures
A43.Generally there are four steps involved in obtaining CMS approval of a WCMSA. These steps are explained in more detail in the Q & A 44-63. Note, there is no CMS approval process in place for LMSAs. The four general steps are:
- a. analysis of the claim and medical information in order to determine the amount of money required to fund the MSA
- b. negotiation of a tentative settlement and preparation of draft settlement documents to settle the workers’ compensation or personal injury liability case, incorporating terms for creation and administration of the MSA (CMS is not a party to the settlement)
- c. obtaining approval from CMS for the amount of the proposed WCMSA (no approval process in place for LMSAs), and
- d. finalizing the settlement and funding the MSA
See, WCMSA Reference Guide §7.0
A44. Initially a function of the CMS Regional Office where there was no uniform established guidelines for CMS review of a WCMSA the concept of a “review contractor” began on November 10, 2003 when CMS contracted with a “joint venture” contractor ( The Workers’ Compensation Review Center – Joint Venture of 10830 Guilford Road, Ste. 307, Annapolis Junction, MD 20701) who had the initial responsibility to review pre-October 1, 2003, cases (which CMS referred to as “the backlog”). The cases were sent by the joint contractor to the CMS Regional Offices with a recommendation or additional information request. Once the joint venture contractor had provided a recommendation to the CMS Regional Office, acknowledgment of the receipt of the WCMSA proposal was sent to the submitter, usually within a 2 – 3 day period, or additional information was requested from the submitter. This role then was expanded to include review of all WCMSA proposals regardless of the date of submission to CMS. The purpose of the joint venture contractor was to assist the CMS Regional offices in their WCMSA review process, insure adequacy of the WCMSA funds to insure Medicare’s interests were properly considered, maintain national consistency in review procedures, streamline the WCMSA review process and to complete the review process in a more timely fashion.
Today, as of July 1, 2012, the current workers’ compensation review contractor (WCRC) is Provider Resources, Inc., 2005 West 8th Street, Ste. 208, Erie, PA 16505 (1-855-280-3550, 1-814-480-8732, www.provider-resourcews.com) which acts as the sole reviewer of WCMSA proposals. This was an initial one year contract ($5,124,084) with four subsequent 12 month option periods which could be exercised at CMS’ discretion.
The WCRC performs an independent review of the adequacy of the medical and prescription drug and durable medical equipment costs included in the submitted WCMSA proposal, and prepares a recommendation to CMS about the proposal and whether it adequately considers Medicare’s interests. The WCRC reviewer considers all evidence provided in the submission. This includes any treatment records, physician dispensed medication records, payment records, court orders, treatment guidelines, or applicable statutes that were attached to the submission. See, WCMSA Reference Guide, §9.4.4 Step 9.
The WCRC will always price the case at 100% of the future costs related to the claim. CMS does not recognize any reduction of future medical items and services or prescription drug costs related to the claim that result due to the claim being settled for less than full value or in the case of a LMSA due to comparative negligence. See, WCMSA Reference Guide, §9.4.4 Step 9(see also, Q & A 81).
The WCRC upon reviewing each WCMSA proposal recommends a WCMSA funding amount which is then reviewed by CMS Regional Office for a final determination as to the recommended WCMSA amount.
A45. It depends. It is unnecessary for the beneficiary to establish a MSA as a result of the settlement or judgment if all of the following are true:
- a. the facts of the case demonstrate that the individual is only being compensated for past medical expenses (i.e., for medical services or prescription drug charges furnished prior to the settlement)
- b. there is no evidence that the individual is attempting to maximize the other aspects of the settlement (e.g., the lost wages and disability portions of the settlement) to Medicare’s detriment
- c. the individual’s treating physician(s) certifies in writing that to a reasonable degree of medical probability the beneficiary will no longer require any Medicare payable or reimbursable medical services or prescription drug charges due to the work or accident related injury or illness. Note: a similar opinion only by an independent medical evaluator will not satisfy the requirement that the written opinion be that of a treating physician; and
- d. the beneficiary signs an Informed Consent memorializing the advise given by their counsel as to the purpose of a MSA, options for use of a MSA and the risk which the beneficiary may face should a MSA not be utilized
See, WCMSA Reference Guide, §4.2( see also, Q & A 32 regarding open-medical settlements)
A46. No. There are no statutory or regulatory provisions requiring that any party submit a MSA proposal to CMS for review. If a chooses to use CMS’ MSA review process, CMS requires that the party comply with CMS’ established policies and procedures in order to obtain approval.
Nor will the practitioner find any statute or regulation that mandates the establishment or use of a MSA in any particular format or mandate prior approval by CMS of the MSA. See, WCMSA Reference Guide, §1.0.
Contrary to some defense counsel assertions the MMSEA(Q & A 4) contains absolutely no reference to or regulations for the use, creation, administration or referral of a MSA to CMS whether it be in workers’ compensation or liability claims.
Comment: : Having said that the utilization of a MSA to protect a beneficiary’s current or future Medicare coverage is a separate and distinct issue to resolve independently of whether a MSA meets current CMS review thresholds. Not referring a MSA is not the same as not necessarily needing a MSA.
What is true, however, is that a use of a MSA is the best tool available to memorialize and document that Medicare has been given due consideration in a settlement. Additionally, approval of a submitted MSA is the only method to achieve certainty as to what Medicare’s position will be as to when Medicare will pay for work or accident related medical services and prescription drug costs.
While there is no such authority for the use of or referral of a WCMSA the practical reality is that it will be the beneficiary who suffers when a MSA is not utilized when the facts indicate there will be future work related medical services and/or prescription drug costs since Medicare may well deny coverage and payment up to the gross settlement amount for future work related medical services and prescription drug bills leaving the client with the long arduous process of appealing a Medicare payment denial to the ALJ.
A beneficiary may consider seeking CMS approval of a proposed MSA amount for a variety of reasons. The primary benefit is the certainty associated with CMS reviewing and approving the proposed amount with respect to the amount that must be properly spent. It is important to note, however, that CMS approval of a proposed WCMSA amount is not required. See, WCMSA Reference Guide, §4.1.
If a proposed WCMSA amount meets the workload review thresholds ( Q & A 51) the proposal can be submitted to CMS for approval. CMS reviews proposed WCMSA amounts in order to determine if the proposed amount is sufficient to cover future claim related medical and/or prescription expenses. There are no current review thresholds established by CMS for LMSAs. See, WCMSA Reference Guide §8.0.
If the parties to a workers’ compensation settlement stipulate a WCMSA amount but do not receive CMS approval, then CMS is not bound by the amount stipulated by the parties, and CMS may refuse to pay for future claim related medical expenses, even if they would ordinarily have been payable or otherwise reimbursable by Medicare.
However, if CMS approves the WCMSA amount and that amount is later properly depleted, Medicare will pay Medicare payable or otherwise reimbursable claim related medical services and pharmacy bills regardless of the amount of care the beneficiary continues to require.
Note: A WCMSA amount should not be submitted to CMS when the resolution of the workers’ compensation claim results in the medical portion of the claim being left open—that is, the resolution does not include medical expenses and the WC plan or carrier maintains ongoing responsibility for medicals, i.e., the workers’ compensation carrier or plan will continue to pay for claim-related medical expenses after settlement. (see Q & A 32).
A47. No. Having said that the analysis of future accident or work related medical services and prescription drug changes which are payable or otherwise reimbursable under Medicare requires a special skill set and training. Any individual or entity that prepares the MSA should be certified in this area. Se Q & A 25 for a discussion on the components that make up a MSA analysis.
Regardless of whether a party utilizes a formal MSA analysis approach the referral must include an analysis of the future work or accident related medical services and prescription drug charges and provide an explanation as to how the MSA was calculated (see Q & A 25). Note, that CMS does not necessarily consider the MSA as conclusive. CMS may not credit the analysis if there is information that calls the analysis into question for some reason, such as contrary medical evidence, apparent internal conflicts of interest , or if the analysis is not credible on its face. See, WCMSA Reference Guide §6.0.
A48. Yes, but this is not recommended. The parties may proceed with the settlement but the proposed amount of the WCMSA is not binding upon CMS.
The question becomes, however, if CMS does not subsequently provide approval of the proposed WCMSA amount as specified in the settlement and offers a counter proposed WCMSA amount that is higher than WCMSA originally submitted to the WCRC how is the difference funded and who funds it? If proof is not provided CMS that the CMS approved WCMSA amount has been fully funded (by submitting a copy of the final, signed settlement documents indicating the WCMSA amount is the same amount as that recommended by CMS) CMS will deny payment for medical services and prescription drug charges related to the workers’ compensation claim up to the full amount of the settlement. Only the approval of the WCMSA by CMS and the submission of proof that the WCMSA has been funded with the approved amount limits the denial by Medicare of related medical services and prescription drug claims to the amount in the WCMSA. The reader is directed to the Author’s text entitled Practitioner’s Reference Manual To Settlements, Offsets & Set-asides – Second Edition published by Atlantic Law Book Company, West Hartford, Connecticut 06110 with projected release date of November 2015 www.atlanticlawbooks.com/practionersGuide.htm for options available which include Postsettlement approval by CMS – beneficiary funded excess, Post-settlement approval by CMS – respondent funded excess/opt-out, Post-settlement approval by CMS – shared funded excess, and reversionary provisions contemplating a counter-higher CMS approved amount.
A49. Yes. CMS established case voluntary workers’ compensation review thresholds (Q & A 51) and will review a proposed WCMSA and provide a written opinion on which the parties may rely regarding whether the settlement has adequately considered Medicare’s interests pursuant to 42 C.F.R. 411.46. These proposed settlements are handled by the WCRC on a case-by-case basis, as each situation is different. (Q & A 58)
Comment: : Certain CMS Regional Offices are reviewing LMSA proposals. Until such time as CMS promulgates review thresholds for LMSAs the referral of a proposed liability settlement to CMS would suggest an unnecessary exercise given CMS’ current absence of any due process appeal rights to their analysis.
A50. No. CMS will not give an advisory opinion or what CMS refers to as “verification” letters on either (1) the sufficiency of an WCMSA or (2) confirming that approval of an WCMSA is unnecessary where the claim does not meet review thresholds. See, WCMSA Reference Guide, §§4.2, 8.1.
A51. Note: Regardless of the dollar threshold, Medicare beneficiaries should always consider Medicare’s interest in all workers’ compensation cases and ensure that Medicare is secondary to workers’ compensation. See, WCMSA Reference Guide, §14.0.
The thresholds for review of a WCMSA are only CMS “workload” review thresholds, not substantive dollar or “safe harbor” thresholds for complying with MSP provisions. Under the MSP provisions, Medicare is always secondary to workers’ compensation and other insurance such as no fault and liability insurance. Accordingly, all injured parties, whether resolving a workers’ compensation or personal injury claim must consider Medicare’s interest when settling the claim. The current review thresholds are subject to adjustment and CMS reserves the right to modify these guidelines. See, WCMSA Reference Guide §8.1.
For liability claims:
Currently there are no established CMS review thresholds for liability settlements. There are some CMS Regional Offices that may review a LMSA but as with all submissions this would be entirely voluntary on the part of the submitter.
For workers’ compensation claims:
According to CMS, when the Patel Ju1y 23, 2001 memorandum (Q & A 5) was released, it established review thresholds for workers’ compensation cases settled by injured workers who were not yet Medicare beneficiaries. This was done in order to organize and prioritize workloads for CMS’ Regional Offices and to convey to those offices that it is not in Medicare’s best interests to review workers’ compensation settlements that do not meet these review thresholds.
CMS will review a proposed settlement including a WCMSA that meets these thresholds and will give a written opinion upon which the beneficiary and parties may rely, regarding whether the workers’ compensation settlement has adequately considered Medicare’s interests pursuant to 42 C.F.R. 411.46.
ONCE THRESHOLD REVIEW CRITERIA ARE MET AND APPROVAL OF AN WCMSA OBTAINED THIS WILL BE PRIMA FACIE EVIDENCE THAT MEDICARE’S INTERESTS HAVE BEEN ADEQUATELY CONSIDERED. THE BENEFICIARY WILL THEN HAVE ASSURANCE THAT THE BENEFICIARY’S FUTURE ENTITLEMENT OR CONTINUED ENTITLEMENT TO MEDICARE COVERAGE WILL NOT BE JEOPARDIZED. FINALLY, FROM A PRACTITIONER’S VIEWPOINT, ADHERENCE TO CMS’ THRESHOLD REVIEW CRITERIA WILL AVOID POTENTIAL MALPRACTICE MISSTEPS.
Comment: : While CMS is fond of using the term “protect” when discussing the WCMSA process, e.g., Medicare’s interests must be “protected”, in the opinion of the Author there is no requirement for attorneys to protect the interests of Medicare. Rather, the practitioner’s obligation is to give Medicare’s interests due consideration and in so doing protect the interests of his or her client. All too often in the workers’ compensation arena the fact that a particular claim meets or does not meet the published CMS review criteria is believed to answer a collateral yet independent analysis as to whether a WCMSA is needed or not. This is a falsehood since all settlements must give due consideration to Medicare’s future interests. Presently the best tool available to do this is to consider using, and if appropriate submitting, a WCMSA prepared by an independent objective specialist in the area.
Approval of a WCMSA may be sought from CMS under the following conditions:
- 1. For Current Medicare Beneficiaries (Class I):
If the beneficiary is a current Medicare beneficiary and the “total settlement amount” is greater than $25,000 referral is indicated. Between 7-11-05 and 4-25-06 this threshold was $10,000. There was no minimum threshold prior to 7-11-05.
“Total settlement amount” includes, but is not limited to (a) all future indemnity benefits e.g., temporary total, temporary partial, permanent partial, etc…, (b) attorney fees and costs, (c) all future work or accident related medical service or prescription drug charges payable or otherwise reimbursable by Medicare (d) all future work or accident related medical service or prescription drug charges not covered by Medicare, (e) any repayment of any Medicare conditional payments or other liens, (f) any amounts forgiven by the carrier, and (g) the value of any previously settled portion of the claim.
Comment: : It is the Author’s opinion that “previously settled portion of the workers’ compensation claim” can be problematic.
In those cases where the indemnity portion of the workers’ compensation claim is settled leaving the medical component “open” and this medical component later settles then the previous indemnity settlement value would then be added to the new medical component settlement value in order to establish the gross settlement value. It is the combined new gross settlement value that is matched to the thresholds to determine whether the case now is eligible for CMS review. Another problem area is the fact that many aspects of a workers’ compensation claim may be “settled” or “compromised” during the life of a claim. To include the value of any previously settled portion of a workers’ compensation claim is unworkable. What does this mean? Does it include a commutation of permanent partial impairment benefits? What of contested compensation rates? In the opinion of the Author it would be appropriate to include a previously settled portion of the workers’ compensation claim if it was contemporaneous to the full and final settlement e.g., the workers’ compensation carrier will resolve outstanding medical liens over and above the amount it will pay in settlement. It would also be appropriate to include truly “settled” portions of a case e.g., where benefits are compromised up to a certain date in time or where certain body parts are covered but only for a period of time. Otherwise, only those amounts paid as gross settlement proceeds should properly be included.
- 2. For Prospective Medicare Beneficiaries (Class II):To the extent a workers’ compensation settlement meets both of the following criteria a referral to CMS is indicated:
- 1. the “total settlement amount” payable over the duration of the settlement agreement (not the discounted present cash value of the settlement) is greater than $250,000, and
- 2. there is a “reasonable expectation” that the beneficiary will become a Medicare beneficiary within 30 months of the settlement date.
- a. the beneficiary has actually applied for SSDIB
- b. the beneficiary has applied for SSDIB but has been denied and the beneficiary anticipates or intends to appeal the denial
- c. the beneficiary is in the process of appealing and/or refiling a new application for SSDIB
- d. the beneficiary is 62½ years of age. A beneficiary who has reached the age of 62½ will automatically meet this component of the threshold regardless of the beneficiary’s disability status as there are 30 months before the beneficiary reaches age 65 which is the automatic age one is entitled to Medicare coverage.
- e. the beneficiary has End Stage Renal Disease (ESRD) but does not yet qualify for Medicare based on ESRD (3month waiting period after dialysis or kidney transplant)
- f. the beneficiary has Lou Gehrig’s disease (Amyotrophic Lateral Sclerosis or “ALS”) which has no waiting period
To the extent a workers’ compensation settlement meets both of the following criteria a referral to CMS is indicated:
A “reasonable expectation” of Medicare enrollment is not an extreme, immoderate, or excessive chance that the beneficiary will become a Medicare beneficiary. Rather a reasonable expectation of Medicare entitlement can be anticipated where one of the following fact patterns has been established:
As to items a-c the practitioner must be knowledgeable in Social Security disability eligibility criteria in order to make a determination as to whether the work or accident related injury or illness, coupled with any other disability or impairment the beneficiary may have, meets or equal one of the “Listings” necessary to qualify for SSDIB benefits or whether the beneficiary would be found disabled under the “Grid”.
Note that CMS has an internal non-published guideline that provides that if the beneficiary will be Medicare eligible within 120 days of the submission date or 60 days of the MSA pricing date then CMS will consider the beneficiary “Medicare eligible” and impose the $25,000 threshold rather than the $250,000 threshold.
Comment: : Since everything else is black and white in CMS’s eyes this “guideline” makes no equitable sense. This should be a light switch….not a dimmer switch…either the beneficiary is Medicare eligible on the date of settlement or there is a reasonable likelihood that s/he will be Medicare entitled within 30 months of settlement. There should be no 60-120 day fudge factor!
Caveat: This answer came from the Patel July 23, 2001 Regional Administrators Memorandum (Q & A 5). It was “clarified” in the Walters July 11, 2005 Regional Administrators Memorandum (Q & A 5). This is an example of why the CMS referral process is so confusing and why proper federal regulation is necessary.
A52. Version 7-23-01 When an beneficiary who is not a Medicare entitled individual and does not have a reasonable expectation of becoming a Medicare entitled individual within 30 months of a settlement and the settlement does not meet both thresholds ($250,000/reasonable expectation) Medicare will make payment for work related medical or prescription drug charges that are otherwise payable or reimbursable under Medicare once the beneficiary enrolls in Medicare. CMS assumes that when a non-Medicare eligible beneficiary’s workers’ compensation settlement does not meet the 30-month and $250,000 thresholds, typically that beneficiary will completely exhaust the settlement by the time Medicare e1igibility is reached.
Version 7-11-05: The thresholds for review of a WCMSA proposal are only CMS workload review thresholds, not substantive dollar or “safe harbor” thresholds for complying with the Medicare Secondary Payer law. Under the Medicare Secondary Payer provisions, Medicare is always secondary to workers’ compensation and other insurance such as no-fault and liability insurance. Accordingly, all beneficiaries must consider and protect Medicare’s interest when settling any workers’ compensation case; even if review thresholds are not met, Medicare’s interests must always be considered.
Caveat: This answer is from the 5-23-03 Grissom Regional Administrators Memorandum(Q& A 5) and must be read in context with the Q & A 52 discussion above and particularly the Walters 7-11-05 Memorandum
A53. Yes. For workers’ compensation settlements that do not meet the thresholds, Medicare will make payments for workers’ compensation related medical services and prescription drug charges that are payable or otherwise reimbursable under Medicare, once the beneficiary becomes enrolled in Medicare. This will be done regardless of when the sett1ement actually occurred. However, a reopening of claims (see 42 C.F.R. 405.750 and 405.841) that Medicare previously denied for the beneficiary will not be granted, nor will CMS change any decisions already made with respect to settlements which pre-date July 23, 2001. According to CMS, when the Patel Ju1y 23, 2001 memorandum was released, it established review thresholds for workers’ compensation cases settled by a beneficiary who was not yet a Medicare beneficiary. This was done in order to organize and prioritize workloads for CMS and to convey to its Regional Offices that it is not in Medicare’s best interests to review workers’ compensation settlements that do not meet the review thresholds.
A54. There are no pleadings or special CMS submission forms to refer a WCMSA to CMS. For an example of what a submission looks like refer to the WCMSA Reference Guide Appendix 4. See, WCMSA Reference Guide, §13.0.
When a WCMSA is submitted for approval, the WCRC must be provided certain documentation available to complete a review of the WCMSA proposal. See Q & A 56 for a list of the documents normally submitted with a WCMSA proposal. See, WCMSA Reference Guide, §10.0.
When CMS first started the WCMSA review process the submission process went something like this:
The settlement proposal with the proposed WCMSA was sent to the CMS Coordination of Benefits Contractor (COBC). The proposal would be directed to the attention of the Regional Office Medicare Secondary Payer Coordinator, who then would forward the inquiry to the appropriate CMS Regional Office. WCMSA responsibilities were generally, but not always, assigned based upon CMS Regional Office responsibility for contractor oversight over the lead fiscal intermediary for workers’ compensation recoveries for a particular state. This could or could not have been the same CMS Regional Office as the one with general responsibilities for a particular state.
Beginning in 2004, in an effort to create unified criteria for submission and pricing of the WCMSA, direct submission to the CMS Regional Office was no longer allowed and the WCMSA was instead submitted to the Medicare Coordination of Benefits Contractor (COBC) in New York. Beginning on August 27, 2007 all WCMSA referrals were sent to Detroit and more recently to Oklahoma. If the WCMSA was sent directly to the CMS Regional Office, the CMS Regional Office would send it on to the COBC contractor.
Today, the process is different. The COBC has been recreated as the BCRC. The BCRC catalogs the WCMSA referral in a centralized case control system. The BCRC does not make the actual determinations as to the adequacy of the WCMSA. Purportedly, one of the purposes of the centralized case control system is to establish the average life-span of the MSA, the experience with medical fee schedules versus actual charges, and similar questions. The data will eventually be made public but there is no time-frame for release of this data.
A WCMSA can be submitted in one of two ways: electronically through the WCMSAP on the internet, or by paper submission through the mail. Submission via the WCMSAP is preferred. WCMSAs are handled in the order they are received regardless of the submission method. See, WCMSA Reference Guide, §11.0.
When a WCMSA proposal is submitted on paper or CD, the Benefits Coordination & Recovery Center (BCRC) transfers it to CMS’ computerized system and checks it for completeness. Then it is ready to be reviewed by the WCRC. Proposals submitted online via the WCMSAP go directly to the WCRC for review. Either the BCRC or the WCRC may request more information from the submitter as necessary. The WCRC applies CMS’ criteria in reviewing proposals, and forwards the proposals along with a recommendation on the appropriate funding amount to the assigned CMS Regional Office (RO) for a final determination.
Here is an illustration of the submission process and all of the entities involved. A single direction arrow indicates one-way communication. A double-direction arrow indicates two-way communication. More detailed information about this process immediately follows this diagram.

For WCMSA submissions by hard copy or CD the BCRC manually prepares, sorts and scans all eligible WCMSA proposals including all documentation received and inputs it into CMS’ computerized system and checks it for completeness. At that point the WCMSA is ready to be reviewed by the WCRC.
WCMSAs submitted online via the WCMSAP go directly to the WCRC for review.
The WCRC review process varies depending on the method of submission. For hard copy submissions, the BCRC performs the checks for completeness, makes requests for additional information, and it manually prepares, sorts, and scans all eligible WCMSA proposals, including all documentation received, into the CMS system used to report and track WCMSA cases. See, WCMSA Reference Guide, §§9.2, 9.3.
For WCMASP submissions, no document scanning and entry is necessary. The WCMSAP will also check CMS’ records for a death date for the beneficiary at the time of submission. Any requests for additional information or for proof that the beneficiary is living will be communicated to the submitter, with an email notification. See, WCMSA Reference Guide, §9.3.
The BCRC’s role, therefore, in this process is limited to preparing and developing the case. Once the case is ready, the WCRC performs the initial review of the proposal.
Once the WCRC has completed its review it will (1) advise the submitting party that the referral does not meet review thresholds, (2) request additional information from the submitting party, (3) respond with a counter proposal representing a different MSA amount (higher or lower) than proposed (4) approve the WCMSA as submitted, or (5) reject the WCMSA.
A. Referring the WCMSA to CMS by Hard Copy or CD
If the CMS referral is made by hard copy or CD it is sent to:
WCMSA Proposal/Final Settlement
P.O. Box 138899
Oklahoma City, OK 73113-8899
BCRC will acknowledge the receipt of the WCMSA referral by letter. See, WCMSA Reference Guide, §11.2.
B. Referring the WCMSA to CMS via the WCMSAP
Recognizing the significant delays inherent in a manual processing of thousands of WCMSAs through the mail via the BCRC CMS has implemented the Workers Compensation Medicare Set-Aside Portal or “WCMSAP”.
When a WCMSA case is submitted online via the WCMSAP, case information is electronically transmitted to the CMS system used to report and track WCMSA cases. The submitter will receive an email alert which can only be viewed on the WCMSAP. This alert acknowledges that the case was received. See, WCMSA Reference Guide, §9.1.
A55. The WCMSAP was designed to improve the efficiency of the submission process for WCMSAs, including speeding receipt of the proposal by the WCRC, quicker turnaround times for submissions, and case access for the submitter.
Using the WCMASP to submit a case means the submitter no longer has to mail the submission or burn PDF files to a CD for mailing. Instead, the submitter can gather the WCMSA proposal and its supporting documentation for direct upload to the system. This is easier for the submitter, potentially avoids processing complications, and streamlines the process. See, WCMSA Reference Guide, §11.0.
Use of the portal requires the user to be registered as a valid user . To start the registration process go to: www.cob.cms.hhs.gov/WCMSA/.
Additional information may be found at:
www.cms.gov/Medicare/Coordination-of-Benefits-and-Recovery/Workers-Compensation-Medicare-Set-Aside-Arrangements/WCMSAP/WCMSA-Portal.html
A56. Regardless of whether the referral is made by hard copy, CD or by WCMSAP the required information is the same. Note that while LMSAs have no established threshold review levels established it is anticipated a LMSA referral would require similar information.
When submitting a WCMSA for review a “cover letter” is required with the WCMSA submission. It is used to present CMS with a high level overview of all of the information that is included in the WCMSA proposal. It is important to include as much information as possible in the cover letter rather than simply referring to the different sections that are included in the submission. Include all pertinent names, addresses, phone and fax numbers; all demographic information about the beneficiary; all summary numbers and other data for the settlement and the WCMSA. This helps CMS review the proposal more quickly. See, WCMSA Reference Guide, §10.1.
Some helpful hints regarding the submission process:
- a. if you are planning to submit more than 200 pages of information or more than two years of medical records, it is helpful to contact the WCRC first to discuss if it is all needed
- b. do not resubmit previously submitted documents unless the submitter has confirmed that they were not received. If the submitter is unsure what is needed, call the WCRC (toll-free at 1-855-280-3550 between 9am-5pm EST, Monday thru Friday) to see if what the submitter is sending will be sufficient.
- c. respond to letters and telephone requests for information in a timely manner and completely
- d. check the status of the submission via the WCMASP if the submitter has used the WCMSAP. Note that for cases submitted via the WCMSAP, the submitter can review case information any time.
- e. contact the WCRC in regard to the status of a case that was submitted via mail or CD. The submitter should allow 45 business days after the submission of a complete file before contacting the WCRC for a status update. See, WCMSA Reference Guide, §14.0.
The following documentation must be submitted to CMS prior to the approval of any WCMSA.
A. Claimant (Injured Party) Information
- Claimant’s full name
- Claimant’s address and telephone number
- Claimant’s phone number (and fax number, if applicable)
- HICN or SSN
- Claimant’s Gender
- Claimant’s date of birth
- State of jurisdictional venue for the claim
- Rated age
- Life Expectancy Used in WCMSA Proposal
- Claimant’s signed CMS Consent to Release authorization
When submitting the WCMSA, the submitter is required to include the signed Consent to Release authorization, plus any applicable court papers if the Consent to Release authorization is signed by someone other than the beneficiary (for example, a guardian, power of attorney, etc.). Do not include unsigned Consent to Release authorizations or send HIPAA authorizations to obtain medical records from a provider. See, WCMSA Reference Guide, §10.2.
B. Claimant Medicare Entitlement Status
C. Injury Information including description of injury and date of injury or onset of illness
D. Contact Information
- WCMSA submitter information
- WCMSA administrator type
- Claimant’s attorney, if applicable
- Employer
- Employer’s attorney, if applicable
- Workers’ compensation carrier
- Workers’ compensation insurer’s attorney
E. Settlement details including total settlement amount See, WCMSA Reference Guide, §10.5.1.
F. Proposed WCMSA amount
G. Indemnity/medical insurer’s payment history See, WCMSA Reference Guide,
§10.8.
H. Designation of claimant’s disability classification
I. Claimant’s living conditions
J. Current medical treatment See, WCMSA Reference Guide, §10.4.1.
K. Medical treatment records See, WCMSA Reference Guide, §10.7.
L. Current (last two years) prescription drug charges
M. Submit a copy of the WCMSA analysis See, WCMSA Reference Guide, §10.4.2
N. Settlement agreement or proposed court order WCMSA Reference Guide, §10.5.
A57. A development request or letter can come from either the BCRC or WCRC and is a request for missing or additional information.
The five most frequent reasons for development requests by the BCRC or WCRC are:
- a. insufficient or out-of-date medical records
- b. insufficient payment histories, usually because the records do not provide a breakdown for medical, indemnity, or expenses categories
- c. failure to address draft or final settlement agreements and court rulings in the cover letter or elsewhere in the submission
- d. documents referred to in the file are not provided—this usually occurs with court rulings or settlement documents
- e. submissions refer to state statutes or regulations without providing sufficient documentation, i.e., a copy of the statute or regulation, or notice of which statutes or regulations apply to which payments.
See, WCMSA Reference Guide, §9.4.1.1.
A58. After the WCRC case reviewer validates that the injury has been accepted as a compensable injury, the next step is to project related future medical service treatment and prescription drug costs. See, WCMSA Reference Guide, §9.4.3.
These considerations are key to review accuracy:
- a. are there previous injuries that affect the resolution of the accepted injury?
- b. are there underlying medical conditions that will affect the type of future care or the length of care necessary to bring about the best possible outcome?
- c. are there underlying conditions requiring concurrent medications or treatment, but which are not related specifically to this claim?
- d. are non-treating provider reviews and examinations taking precedence over the treating providers’ treatment plan?
- e. are the medical pricing rules used appropriate for the particular region?
The WCRC reviews all of the submitted records and attempts to determine the future care required for the beneficiary, taking into consideration the beneficiary’s specific condition, other comorbidities, and the beneficiary’s past use of healthcare services. WCRC reviewers use evidence based rationale for their determinations, taking into account both published guidelines and current peer-reviewed medical literature. See, WCMSA Reference Guide, §15.2.
The WCRC will consider:
- a. date of entitlement to Medicare
- b. basis for medicare entitlement
- c. type and severity of injury or illness by medical records review
- d. age of the beneficiary
- e. workers’ compensation carrier’s classification of the beneficiary
- f. prior medical and prescription expenses paid by the workers’ compensation carrier due to the injury or illness in the 2 year period after the condition has stabilized
- g. gross settlement amount
- h. WCMSA duration
- I. beneficiary’s living conditions
- k. WCMSA amount
A59. CMS reports that it tries to review and decide WCMSA submissions within a 45-60 day window from the time that all relevant documents are submitted. See, WCMSA Reference Guide, §15.1.
Once the WCMAS has been transmitted to the WCRC the submitter will receive an acknowledgment letter if the submission is by hard copy or CD. If the submitter does not receive an acknowledgment letter the submitter should contact the BCRC at 1-855-796-2627 (TTY/TDD: 1-855-797-2627 for the hearing and speech impaired). If the WCMAS was transmitted via the WCMASP the submitter should check for an email alert. Customer Service Representatives are available Monday through Friday, from 8:00 a.m. to 8:00 p.m. Eastern Time, except holidays.
When the WCRC completes its review and recommendation, the case is sent to the CMS Regional Office assigned to the case based on the beneficiary’s state of residence. Although the CMS assignment is based on the state of residence of the beneficiary, a case may be transferred from one Regional Office to another based on the case’s legal state of venue, or because the Regional Office that the case was originally assigned to no longer processes WCMSA cases.
When the CMS Regional Office (RO) receives the case, they review the WCRC recommendation and make a final determination in the case. The case may not progress to approval for a number of reasons:
a. if the RO determines that the case does not qualify as a WCMSA case because it does not meet CMS’ workload review threshold for any reason, the Regional Office notifies the submitter
b. if the beneficiary dies during the RO review of the submitted WCMSA, and a date of death with supporting documentation, if requested, is provided, then a date of death is entered into the CMS WCMSA system and the case status is changed to “Deceased.”
c. If the RO needs additional information or documentation from the submitter in order to continue processing the WCMSA case, the submitter is notified with a “development” letter. When documentation is received and scanned at the BCRC, the status of the case changes to “Development Received,” and the Regional Office begins the review again. If a response is not received within the allotted time frame (i.e., 30 days for cases submitted to the BCRC, 20 business days for cases submitted on the WCMSAP), the case is closed for lack of response.
If a response is received after the case is closed, the file will automatically be reopened once the requested information is received, however, it will be treated as a new submission. The review process begins again and the submitter should receive a response within 45-60 days from the WCRC’s receipt of the requested information. It is, therefore, incumbent upon the submitter to make a complete initial referral, including all the requisite information, in order to expedite the referral process.
d. the RO may determine that the case should be closed. This can happen for a number of reasons, including: the parties are no longer settling, the case should be Black Lung instead of workers’ compensation, the case is a personal injury liability case rather than workers’ compensation case, or the submitter has failed to submit necessary information after repeated development requests. The submitter is notified of the case closure.
e. Approve the WCMSA as submitted. If the recommended WCMSA amount (which is a combined total of medical services and prescription medication costs) is within 5% of the submitter’s total proposed WCMSA amount, the WCRC recommendation is approval of the submitter’s proposed amount. In structured cases, the seed amount is separately calculated. If the recommended initial deposit is within 5% of the submitter’s initial deposit, the WCRC recommendation is approval based upon the submitter’s proposed seed amount. See, WCMSA Reference Guide, §9.4.4 Step 10.
f. Approve the WCMSA with a different amount than originally proposed (counter-higher or counter-lower). The WCRC reviewer will provide a detailed decision rationale when there is a counter higher or counter lower determination.
If the beneficiary is living, the case meets workload review thresholds, any needed development has been received, and the case is not closed for other reasons, the RO reviews the WCRC’s recommendation and makes a determination as to the final CMS approved WCMSA amount. When the final WCMSA amount is determined by the RO, the RO approves the case and the submitter is notified.
After receiving the final approved settlement agreement, according to the applicable state law, the RO updates Medicare’s records with the final settlement date. A case may be re-reviewed once completed, but Medicare’s records will not change until the new final determination is issued. Only then is the disposition recorded in Medicare’s system.
See, WCMSA Reference Guide, §§9.5, 9.6, 12.0.
A60. To check the status of a WCMSA proposal submitted via the WCMASP:
Log in to the WCMASP at www.cob.cms.hhs.gov/WCMSA/ and check the case listings then case status. ( Note: The WCMSAP will only display case information, including case status, for those cases that were submitted through the WCMASP).
To check the status of a WCMSA proposal submitted by hard copy or CD:
Call the WCRC at 855-280-3550.
A61. CMS will not monitor the disbursements from the WCMSA until the beneficiary becomes Medicare-eligible (a beneficiary). However, if the practitioner has incorporated a WCMSA as part of the settlement, the workers’ compensation related medical expenses should be paid from the WCMSA even before the claimant becomes a Medicare beneficiary. Medicare beneficiaries and individuals who are not yet beneficiaries follow the same attestation accounting reporting rules as described in Q & A 41g. See, WCMSA Reference Guide, §18.0.
A62. CMS’ Division of Benefit Coordination has established a “system of records” SOR #09-70- 0537 (published in the Federal Register Vol. 70. No. 242 (12-19-05) which has as its primary purpose to maintain a file of individuals who were injured while employed, not currently Medicare beneficiaries, and who have a WCMSA (either approved or not approved) as part of a workers’ compensation settlement.
This SOR provides the legal authority to maintain records on beneficiaries that are not yet enrolled in Medicare. It also allows CMS to disclose to “another Federal and/or state agency, agency of a state government, an agency established by state law, or its fiscal agent to disclose individual specific information contained in its “Common Working File”. This file includes the following information:
- a. beneficiary’s name and HICN number
- b. date of injury or illness
- c. ISD-9/10 code(s): If codes are not readily available the CMS Regional Office or WCMSA must include a description of the illness/ injury
- d. an indication as to type of WCMSA administration e.g., self-administered or professionally administered
- e. beneficiary’s attorney information
The CMS Regional Office will be responsible for maintaining or “housing” the records for every WCMSA on which the CMS Regional Office has provided a written opinion. According to CMS, these records will not subject to Freedom of Information Act requests and may not be disseminated to the public.
A63. Historically CMS sought to review and make a decision regarding a proposed WCMSA within 60 days from the time that all necessary/required documentation had been submitted to CMS. Prior to the current review contractor Provider Resources, Inc. becoming the WCRC wait times could exceed 90-180 days or more.
A64. No. If the WCRC does not believe the proposed WCMSA adequately considers Medicare’s interests it will send the practitioner a counter proposal along with its analysis in support of the counter proposal. This counter proposal can be higher or lower than the proposed WCMSA amount originally submitted. Most times the practitioner’s first notice of the rejection of the recommended WCMSA is with the approval letter sent (or posted on the WCMSAP) by CMS indicating the counter proposed WCMSA amount. There is no formal appeals process.
While there is no direct right of appeal to a WCRC counter proposal the practitioner can request a “re-review” of the counter proposal. This was previously called a “Clarification” or “Challenge”. There is no formal pleading form required. The submitter may request a “re-review” of the approved WCMSA amount when the submitter disagrees with CMS’ decision if:
- a. the submitter believes CMS’ determination contains obvious mistakes (e.g., a mathematical error or failure to recognize medical records already submitted showing a surgery, priced by CMS, that has already occurred); or
- b. the submitter believes there is additional evidence, not previously considered by CMS, which was dated prior to the submission date of the original proposal and which warrants a change in CMS’ determination
The re-review request can be filed through the WCMSAP or mailed to:
WCMSA Proposal/Final Settlement
P.O. Box 138899
Oklahoma City, OK, 73113-8899
BCRC will consider this re-review as a new referral and will process it in order of receipt. The review process by BCRC will most likely take 60-90 days once the new medical evidence is received by BCRC. Presently there is no further “appeal” to an adverse BCRC response as a result of a re-review.
Whether to file a re-review request to a counter proposal requires comparing the variance between the WCMSA dollar amounts originally proposed and those counter proposed and weighing that against the additional time necessary to file and await a decision from BCRC, as well as, considering any additional attorney fees and medical report fees incurred in order to file the request for re-review.
The CMS counter proposal has to be reviewed by the attending physician(s) and specific rebuttal provided as to the reasonableness and necessity of the medical services or procedures or prescription drug charges contained in the counter proposal.
See, WCMSA Reference Guide, §16.0.
Are there any other options? Yes but each carriers its own risks. These include renegotiation, rejection, the open medical settlement and the reversionary set-aside. Each is discussed in the Author’s text entitled Practitioner’s Reference Manual To Settlements, Offsets & Set-asides – Second Edition published by Atlantic Law Book Company, West Hartford, Connecticut 06110 www.atlanticlawbooks.com/practionersGuide.htm (with projected release date of November 2015).
Disbursements from the WCMSA
A65. WCMSA funds may only be used to pay for those medical services or prescription drug charges associated with the workers’ compensation claim being settled that would normally be payable or otherwise reimbursable by Medicare. Examples of some items that Medicare does not pay for are: acupuncture, routine dental care, eyeglasses or hearing aids; therefore, these items cannot be paid from the WCMSA even if related to the Workers’ Compensation claim. For a more extensive list of services not covered by Medicare, the practitioner should obtain a copy of the booklet “Medicare & You” from a local Social Security office or from www.medicare.gov/medicare-and-you/medicare-and-you.html. See, WCMSA Reference Guide, §17.3.
The administrator of a MSA may also disburse certain costs that are directly related to the MSA account:
- a. document copying charges
- b. mailing fees/postage
- c. any banking fees related to the account
- d. income tax on interest income from the set-aside account (see, Q & A 39)
A66. Yes. As of July 11, 2005, for a claimant who is not yet a Medicare beneficiary and for whom CMS has approved a WCMSA, the WCMSA may be used prior to becoming Medicare entitled because the accepted WCMSA amount was priced based on the date of the expected settlement. See, WCMSA Reference Guide, §17.4.2. However, use of the WCMSA is limited to medical services (and as of January 1, 2006 prescription drug charges) that are related to the workers’ compensation settlement that would be payable or otherwise reimbursable by Medicare if the claimant was a Medicare beneficiary. The same requirements that existing Medicare beneficiaries follow for reporting and administration are to be used by a claimant who is not a Medicare beneficiary. The beneficiary’s Medicare entitlement status may change over time. However, the beneficiary’s use of the WCMSA should not.
Even if there is no CMS approved MSA, any funds from a workers’ compensation or personal injury settlement attributable to future medical services and prescription drug charges that are remaining at the time a claimant becomes a Medicare beneficiary must be used for Medicare payable or otherwise reimbursable medical services and prescription drug charges related to the workers’ compensation or personal injury settlement until such funds are properly depleted. Only then will Medicare pay for Medicare covered services and prescription drug charges related to the workers’ compensation claim or settlement.
Prior to July 11, 2005 CMS’ policy was until the claimant actually became entitled to Medicare, the WCMSA could not be used to pay the beneficiary’s work related medical or prescription expenses. Once the beneficiary actually became entitled to Medicare the beneficiary was permitted to make payments for the beneficiary’s medical services and prescription drug charges from the WCMSA that would otherwise be payable or reimbursable by Medicare. See, WCMAS Reference Guide, §17.4.
A67. If the BCRC monitoring the beneficiary’s case discovers that payments from the WCMSA have been used to pay for medical services or prescription drug charges that are not payable or otherwise reimbursable by Medicare or for unauthorized expenses paid from the WCMSA(Q & A 65) which arose out of the administration of the WCMSA then Medicare will not pay claims pending its investigation. The BCRC must provide the evidence of the unauthorized expenditures to the CMS Regional Office for investigation. If the CMS Regional Office determines that the expenditures were contrary to the CMS Regional Office’s written opinion on the sufficiency of the WCMSA then the CMS Regional Office will notify the administrator of the WCMSA that CMS Regional Office’s approval of the WCMSA is withdrawn until such time as the funds used for non- Medicare expenses or unauthorized administrative expenses are restored to the WCMSA.
A68. There are two distinct methods for providers, physicians and other suppliers to obtain payment for workers’ compensation covered medical services when funds are held in a WCMSA. Determining which payment method applies depends on whether the WCMSA was calculated using either full actual charges or a workers’ compensation State fee schedule. In no case is the payment from the WCMSA based on Medicare approved rates.
If the WCMSA is based upon a State fee schedule physicians and other suppliers will be paid based on what would normally be payable under that State’s workers’ compensation fee schedule. Accordingly, providers, physicians and other suppliers would not be permitted to bill the medical services component of the WCMSA more than the State’s workers’ compensation fee schedule rate. For example, if a provider’s full charge for a particular service is $100 and the workers’ compensation carrier normally pays $65.00 for that particular service, then the WCMSA should only pay $65.00 and the provider can only bill $65.00.
However, when the WCMSA does not contain specific provisions ensuring that the WCMSA cannot be charged more than what would normally be payable under the State’s workers’ compensation fee schedule, then providers, physicians and other suppliers are permitted to be billed and to be paid the full actual charges.
Comment: Realistically, use of the State’s workers’ compensation fee schedule is improbable with a self-administered MSA since the beneficiary does not have ready access to these state fee schedules and if they did would probably not properly interpret them. A beneficiary who intends to self-administer the WCMSA should investigate commercial vendors who provide “selfhelp” services or in the alternative consider utilization of a professional administrator knowledgeable in Medicare coverage and coding, as well as, the State’s workers’ compensation fee schedules. Additionally, since the case has now been settled and the State’s workers’ compensation adjudicatory body or the civil court no longer has jurisdiction over the matter, fee disputes would seem not to be readily resolvable short of an appeal to the ALJ.
A69. CMS requires WCMSA pharmacy charges to be calculated using RedBook® average wholesale prices (AWP). Many of the prescription drugs can be purchased at big box pharmacies at below AWP. CMS has not addressed either the contingency that a prescription drug cannot be purchased for at least the AWP used to calculate the WCMSA or addressed the issue of inflationary pressures on pharmaceutical drugs. Accordingly there is no mechanism in the WCMSA to address the contingency that a drug cannot be purchased for the price listed in the WCMSA.
Comment: Certainly if the drug can be purchased below AWP a rational approach would be to do so and thereby preserve prescription funds for the future. In the case of a drug that cannot be purchased at or below AWP, and the drug is one that has been listed in the WCMSA it is my opinion that the WCMSA can be extended to pay the increased cost of the drug. CMS has not addressed the issue of whether the WCMSA can pay for a new drug which is deemed by the treating physician to be related to the work or accident related and deemed medically reasonable and necessary by the treating physician. It is recommended the practitioner call the BCRC and inquire.
A70. When providers, physicians and other suppliers submit claims to Medicare associated with the beneficiary’s work or accident related injury or illness, Medicare claims processing contractors may deny those claims due to an existing reported workers’ compensation or liability claim under the MMSEA or due to an established MSA and instruct the submitting party to seek payment from the MSA.
However, when a provider, physician or other supplier submits any claims that are for injuries or illnesses that are not work or accident related, then the BCRC should process those claims like they would any other claim for Medicare payment.
On the other side of the isle, when the MSA administrator refuses to make payment on a provider’s, physician’s or other supplier’s claim because the MSA administrator asserts the medical services or prescription drug charges are for injuries or illnesses that are not work or accident related (or for any other reason), and the provider, physician or other supplier, subsequent to the administrator’s denial, submits the claim to Medicare, then the BCRC should consult CMS in order to determine whether Medicare should pay the claim. If a determination to deny the claim is made then Medicare’s regular administrative appeals process for claim denials would apply to the claim.
Duration, Depletion & Termination of the MSA
A71. Maybe… To consider Medicare’s interest, a MSA should be funded based on:
- a. the life expectancy of the beneficiary (based upon the actual or rated age)
- b. a lesser period of time if the jurisdictional State law specifically limits the length of time the workers’ compensation carrier is responsible for work related medical services or prescription drug charges; or
- c. specific medical evidence exists which limits Medicare’s exposure due to a terminal illness
For a discussion on “tapering” prescription medications see Q & A 91.
A72. Effective August 25, 2008, once an WCMSA that has been reviewed and approved by CMS has been established the only method of termination is due to the (1) proper depletion of the MSA funds or (2) the death of the beneficiary.
Prior to August 25, 2008 CMS did allow for modification if the treating physician concluded that the beneficiary’s medical condition had substantially improved. The beneficiary could then submit a new WCMSA proposal covering future expected medical services and prescription drug expenses. Such proposals had to justify at least a 25% reduction in the outstanding WCMSA funds. In addition, such a request for a reduction or termination could not be made until at least five years after the initial approval of the WCMSA and was accompanied by all supporting documentation not previously submitted with the original WCMSA proposal. If CMS determined that a 25% or greater reduction was justified, CMS would issue a new approval letter. After CMS issued a new approval letter, any funds in the current MSA in excess of the newly calculated amount could be released to the beneficiary. As with the original decision, CMS’ decision on the new proposal was final and not subject to administrative appeal.
Comment: If a substantial change in circumstances exists there should be no reason for this August 25, 2008 rule change given the purpose of the MSA is to “reasonably” consider Medicare’s interest.
A73. MSAs that are funded by lump sum present less of a problem to administer than structured MSA arrangements. In both the lump sum and structured MSA Medicare does not make any payments for the beneficiary’s Medicare payable or otherwise reimbursable medical services or prescription drug charges until the funds within the MSA have been properly depleted and an accounting confirming same is filed with the BCRC.
However, unlike lump sum funding, structured MSAs are funded with an initial “seed” amount followed by annual “feed” amounts for the life of the beneficiary (or a defined period of years, if state statue provides for). This can create what is known as “temporary depletion”.
If funds for a structured MSA are not depleted during a given period, then these excess funds must be carried forward to the next period. The threshold after which Medicare would begin to pay for expenses related to the claim would then be increased in any subsequent period by the amount of the carry forward. This carry forward process continues until the accumulated carry forward plus the payment for a given year (and accrued interest for those years) is properly depleted. WCMSA Reference Guide, §19.3.1.
Let’s look at an example:
Let’s assume a CMS approved structured MSA is funded with $20,000 per year for Medicare payable or otherwise reimbursable medical services and prescription drug charges on every January 1st over the life of the beneficiary. In the first year of the MSA the beneficiary needed only $15,000 to cover all work or accident related medical and prescription drug expenses. That would mean $5,000 would need to be carried forward into the following year. Then a total of $25,000 ($20,000 annuity payment + $5,000 carry forward) of Medicare payable or otherwise reimbursable work related medical service and prescription drug charges would need to be spent from the MSA before Medicare would again begin to cover work or accident related expenses.
If a structured MSA proves to be under funded for a given period because the funds are properly depleted by the beneficiary’s medical and/or prescription expenses before the period ends, and if CMS receives verification of depletion of both the amount for the period and any available carry forward funds, then Medicare will pay for additional medical expenses incurred during the period. See, WCMSA Reference Guide, §19.3.2.
During this period of temporary depletion the beneficiary may submit work or accident related medical service charges and prescription drug charges which would otherwise be payable or otherwise reimbursable by Medicare, however,
- a. the beneficiary is required to maintain Medicare coverage (Parts A, B, C and/or D)
- b. there is no other valid and collectable health or prescription drug coverage which would be primary to Medicare, and
- c. the beneficiary is responsible for applicable Medicare co-pays, coinsurance and deductibles provisions during this temporary depletion period
Besides notifying the BCRC of temporary depletion the administrator must also now notify the medical provider(s) and pharmacy(s) that for the remainder of the year Medicare (and/or Part D plan, if applicable) will again assume the role of primary payer in lieu of the MSA. Once the next annuity feed is received the roles are again reversed and the MSA becomes primary and Medicare secondary.
Most clients lack this type of sophistication and failing to properly communicate this temporary depletion and shifting financial responsibility which accompanies it, can result in Medicare not picking up payments in a prompt fashion. See, WCMSA Reference Guide, §19.1.
A74. Residual Secondary Payment
A “residual” secondary payment is defined by CMS as a payment Medicare makes on a claim where available funds have been properly depleted from the WCMSA or responsibility for payment terminates mid-service. As of January 4, 2016 Medicare may make a residual secondary payment in situation where ongoing responsibility for medical payments terminate or deplete or a WCMSA depletes while a beneficiary is admitted to a facility or following a physician or supplier visit, and the claim is not fully paid by the WCMSA. See, www.cms.gov/Regulations-and- Guidance/Guidance/Transmittals/Downloads/R113MSP.pdf.
A75. Once CMS and the BCRC responsible for monitoring the beneficiary’s case confirm that all of the beneficiary’s Medicare submitted claims have been paid, any amount left over in the MSA may be disbursed pursuant the terms the MSA funding mechanism itself which are consistent with:
- a. bank or checking account named beneficiary(s)
- b. in the case of a structured MSA the annuity agreement
- c. if neither a or b apply, then the Last Will and Testament of the beneficiary and if none then according to state succession law
This will involve holding the MSA open for some period after the date of death, as providers, physicians, and other suppliers are permitted to submit their initial bill to Medicare for a period of up to one year after the date of service.
In certain cases, where a conservator has been established either as the MSA administrator or otherwise, or where there is a minor involved, the probate court (or other court of competent jurisdiction) approval may also have to be sought for disbursement of remaining MSA funds. See, WCMSA Reference Guide, §19.2.
Funding, Valuation, Calculation & Reduction of the MSA
A76. No. Beneficiaries are not entitled to release of MSA funds if they lose their Medicare entitlement. However, the funds in the WCMSA may be used for medical expenses specified in the WCMSA until Medicare entitlement is re-established or the WCMSA is properly depleted. Use of the MSA continues to be limited to medical services and prescription drug charges that are due to the work or accident that would otherwise be covered by Medicare if the claimant were a Medicare beneficiary.
CMS will not pay for any medical services or prescription drug charges related to the workers’ compensation claim or settlement until a self-attestation document or, in the case of a professionally administered MSA, a full accounting of all monies expended from the MSA are sent to the BCRC responsible for monitoring the beneficiary’s case. Upon the re-establishment of Medicare entitlement the BCRC will adjust the beneficiary’s common working file to reflect the expenses paid prior to re-establishment of Medicare entitlement. See, WCMSA Reference Guide, §17.4.1.
Comment: If, in fact, the beneficiary’s Medicare entitlement is lost, and there is no reasonable likelihood that it will be re-established then this should constitute a substantial change in circumstances justifying petitioning CMS to dissolve the MSA allowing release of the MSA funds.
A77. The only guidance CMS provides here is that the financial investment vehicle used to house the MSA must be in an “interest bearing account”, separate from any other account such as personal savings or checking. See, WCMSA Reference Guide, §17.2.
Comment: As a general rule the MSA funds must be “liquid”. MSA funds may not be placed in speculative investment products where the principal is not fully guaranteed. This means the MSA must be set up as a dedicated FDIC insured bank, checking or savings account or NCUSIF protected credit union accounts, FDIC insured money market account, FDIC insured CD or FDIC insured bank or U.S. Treasury bills or notes. MSA funds which expose the principal to risk will not be acceptable to CMS. Regardless of where the MSA funds are placed these MSA funds must be separate from any other personal funds available to the beneficiary.
Issues can arise with MSAs which exceed the FDIC insurance limit of $250,000 either because the MSA itself is over $250,000 or the beneficiary has multiple accounts in a single bank which combined exceed the $250,000 limit. This issue should be discussed with the bank chosen by the beneficiary prior to any deposit of MSA funds being made.
A78. No. Initially CMS gave consideration to indexing for inflation as there was a requirement that the MSA be indexed consistent with how Medicare calculates its growth in spending. However, as of October 15, 2004, the MSA does not need to be indexed for inflation and in exchange the WCMSA may not be discounted to present cash value.
A79. No. CMS had at one time contemplated and ultimately rejected a suggestion that an additional allocation within the MSA be provided so that medical services and prescription drug charges that were not covered by Medicare at the time the MSA was submitted to CMS for review, but later become Medicare payable or otherwise reimbursable, be transferred from the amount specified for non-Medicare covered items and services into the MSA.
Comment: It is, however, a prudent course of action to have a separate medical allocation (not a MSA) for non-Medicare covered work or accident related items or for Medicare co-pays, deductibles and coinsurance provisions which may apply to work or accident related medical services and prescription drug charges which the beneficiary may incur in the future and which are related to the injury or illness. This certainly can assist in the calculation of any Social Security Disability offset since this separate medical allocation would, like a MSA, still be deemed an excludable medical expense. These funds do not have to be transferred to the MSA or be included in the annual MSA accounting.
A80. No. The WCRC will always price the case at 100% of the future costs related to the claim. CMS does not recognize any apportionment of future medical items and services or prescription drug costs related to the claim due to a case being settled for less than full value regardless of the reason. See, WCMSA Reference Guide, §9.4.4 Step 9.
A81. Yes. A WCMSA can be established as a lump sum arrangement where the beneficiary accepts a single payment intended to pay for all future medical services and prescription drug charges related to the workers’ compensation claim. When a WCMSA is designated as a lump sum commutation settlement (Q & A 28), Medicare will not make any payments for claim related medical or prescription expenses until all the funds within the WCMSA (including any interest earned on the funds in the MSA) have been completely and properly depleted.. Generally, WCMSAs that are lump sums are easier to monitor than structured arrangements.
A82. Yes. The MSA may be structured whereby an initial fund amount plus periodic funds are deposited into the MSA on a defined schedule (rather than in lump sum) to cover future work or accident related medical services and prescription drug costs which are payable or otherwise reimbursable by Medicare. In a structured MSA, an initial deposit or “seed amount” is followed by periodic payment or “feeds” over the beneficiary’s life expectancy (or shorter period if allowed by state statute). For a discussion on how a structured MSA is calculated see Q & A 83. For a discussion on “temporary depletion” of a structured MSA see Q & A 73.
A83. A structured MSA is calculated based upon the normal life expectancy of the beneficiary or by use of a rated age. If a structure is utilized to fund the MSA it will consist of both “seed’ (initial funding) and “feed” (annual deposit) components. See, WCMSA Reference Guide §5.2.
The “seed” money for the MSA must include an amount equal to cost of the (1) the first surgery and (2) first cost of any durable medical equipment plus (3) the first two years of annual projected medical services and prescription drug charges.
The seed amount is followed by a number of subsequent annual deposits calculated by formula and designated as “annual deposits” or feeds. These annual deposits into the MSA are payable upon a set “anniversary date” which commence one year after the initial funding of the MSA.
The periodic payments payable from an annuity contract can based upon:
a. a “temporary life” contract in which case payments continue for the life of the beneficiary but for no longer than that period of years stated in the annuity contract;
b. a “life only” contract in which case payments continue only for so long as the beneficiary is living; or
c. life only guaranteed payable for “X” years contract in which payments are made for so long as the beneficiary is living but for no less that the period of years stated in the annuity contract.
Note that except where the settlement document provides for a guaranteed period of payment there is no guaranty that upon the death of the beneficiary the heirs or estate will receive any residual annual feed payments from the annuity contract. In the life only, guaranteed payable for “X” years option a designated beneficiary(s) can be named guaranteeing a fixed amount remaining to be paid should the beneficiary die.
Periodic payments can be made monthly, quarterly, semi-annually, annually or at specified dates. Which options are chosen will affect the overall up-front cost of the structured settlement and its total payout over time.
Comment: Consultation with a licensed structured settlement broker chosen by the client is recommended so that the client’s best interests are protected. While it is permissible to allow the insurance carrier’s broker to quote and ultimately place the annuity with a insurance carrier licensed to underwrite and sell annuities the present cash value of the annuity and the method by which it terminates varies and is subject to negotiation.
A84. Yes. Effective October 1, 2008 if the MSA includes the pricing for any implantable device(s) and does not include enough information or if it is determined upon review by the WCRC that an implantable device is recommended for the beneficiary but has not been included in the MSA proposal, the WCRC will utilize its own pricing methodology. If an implantable device is being used or recommended the practitioner should consult with the appropriate physician and include the following information in the MSA analysis:
- a. device, electrodes, receiver manufacturer name
- b. device, electrodes, receiver model # or type
- c. device, electrodes, receiver cost including tax, freight and handling
- d. facility fee, whether inpatient or outpatient, procedure code and cost
- e. surgeon procedure code and cost
- f. anesthesiologist procedure code and cost
- g. programming services procedure code, frequency and cost
- h. other associated costs
Prescription Drugs & Medicare Part D
Note: Medicare’s reference to prescription drugs is limited to those prescription drugs that are for the treatment of the workers’ compensation or personal injury related injury(s) or illness(s), and those where Medicare provides coverage under any one of its formulary plans.
A85. The WCRC reviewer verifies that the prescription drugs included in the MSA analysis are for the direct treatment of the work or accident injury or illness from medical records and pharmacy records. Both the medical and pharmacy records are used to compile a beneficiary’s drug list. If the medical records are more recent than the prescription records, the WCRC will use the medical records to compile the drug list. However, if there are major discrepancies between the medical and pharmacy records, the WCRC will use the pharmacy records to compile the drug list, favoring actual use over possibly incomplete medical records.
a. the WCRC reviewer will validate that prescription drugs ordered and taken in the past two years were directly for treatment of the work or accident injury or illness. The WCRC then compiles a drug list. This list is then used to project future drug costs for the duration of a beneficiary’s life expectancy. The WCRC reviewers must see prescription drug payment records/histories dated within 6 months of the date of any submission.
Specifically, for pharmacy records, the WCRC prefers the following:
- 1. First, the prescription claim records directly from the workers’ compensation insurer. This gives a record of exactly what drugs have been used for the work or accident related injury or illness. This might present on such a form as the National Council for Prescription Drug Programs (NCPDP) Workers’ Compensation/Property and Casualty Claims Form. Many state workers’ compensation programs use these forms to document drug payments
- 2. Pharmacy Benefit Manager prescription claim records or third party administrator (TPA) pharmacy records provide a good sense of the totality of drug usage, especially if the beneficiary goes to multiple pharmacies
- 3. Individual pharmacy claim records are beneficial, but the WCRC is aware that beneficiarys could go to multiple pharmacies. If at any time in the process the WCRC cannot compile an accurate picture of the beneficiary’s drug needs, they will send the submitter a development letter for additional information or records
b. determine if the drug products would be covered under the Medicare Part B or D benefit. This includes assessment of medically accepted indications (drug usage), drug dosage, and drug frequency
c. determine if the beneficiary is taking brand or generic drug products. Where drugs are indicated and the submitter has not priced drugs, or where a submitter prices for a generic drug where there is none, CMS will compare the WCMSA proposal to AWP for brand name drugs. If drugs are indicated, but the medical and other records are silent or unclear about whether a beneficiary is taking a brand or generic drug and both versions exist, then CMS will compare the WCMSA proposal to the generic drug where the submitter has proposed a generic drug, and CMS will compare the WCMSA proposal to the brand name drug where the submitter has proposed a brand name drug or has not proposed a drug at all.
The WCRC prices for generic drugs unless one of the following applies, in which case the WCRC uses brand-name:
- 1. a brand-name drug is in the MSA analysis and there is an indication that the beneficiary is actually taking the brand-name drug. Brand name drugs are only available from one manufacturer, whereas generic drugs are available from multiple manufacturers. In the absence of supporting documentation concerning prices from generic drug manufacturers within the WCMSA submission, CMS will compare generic drugs in the WCMSA proposal and use the lowest priced generic drug as listed in Red Book Drug Reference®.
- 2. a generic is in the MSA analysis, but no generic exists
- 3. a generic is in the MSA analysis, but all the evidence indicates that the beneficiary is taking the brand-name drug
- 4. The beneficiary or beneficiary’s attorney insists on a brand-name drug in writing
- 5. No drugs are indicated in the submitted proposal, but the condition requires certain drugs, or the medical records indicate certain drugs. In this case, the WCRC will default to pricing for brand-name medications
- 6. price all drug products using AWP, with generic drugs being priced at the lowest non-repackaged generic AWP
At any time during the process, if a WCRC reviewer is unsure of drug pricing, indication, or allocation amount, those questions are deferred to a CMS pharmacist or pharmacist’s designee before the case is finalized.
When evaluating drug use, the WCRC reviewers assess the drug dosage, frequency, formulation, patents expiring (see, Q & A 95), newer more expensive drugs, and use of brand-name versus generic drugs. Various drug formulations can vary significantly in cost. It is very important to gain an accurate picture of the specific formulation for an accurate pharmacy allocation.
The WCRC continues to price Part D drug products based on AWP and further based on brand or generic drug pricing. AWP pricing is pulled from a proprietary source, Truven Health Analytics’ Red Book® database. The WCRC uses a program for drug pricing that uses Red Book flat files updated quarterly and monthly. For generic drugs, the WCRC uses the lowest non-repackaged generic drug AWP.
Where multiple spellings and listings of a drug exist, the WCRC will price using the original manufacturer of the original brand name drug for brand, and the lowest price generic drug. The WCRC reviewer will price drugs based on the lowest price from the manufacturer, ignoring prices from any repackagers or distributors.
The WCRC uses a number of resources when determining drug coverage for WCMSAs. WCRC reviewers consult Part D and Part B guidance documents, CMS memorandums, current CMS operating rules, the Part D formulary reference file, and recognized drug compendia to assess drug coverage possibilities.
See, WCMSA Reference Guide, §9.4.6.1.
A86. A “covered” Medicare Part D drug” is a drug that may be dispensed only upon a prescription and that is described in subparagraph (A)(I), (A)(ii), or (A)(iii) of 42 U.S.C. §1396r-8(k)(2), 42 U.S.C.§ 1395w-102(e)(1)(A). For a Part D drug to be covered by Medicare, and thus included properly in a MSA, the drug should be prescribed for an outpatient use that is approved under the FDA, and Cosmetic Act (21 U.S.C.A. § 301 et seq), or supported by one or more citations included or approved for inclusion in any of the compendia described in subsection (g)(1)(B)(I) or 42 U.S.C. §1396r-8.
Effective 6-1-10, for those workers’ compensation settlements effectuated prior to 6-1-10, and where the settlement included non-covered Part D drugs as part of the WCMSA, CMS will consider funds spent for those non-covered Part D drugs by beneficiaries as being an appropriate expenditure of funds from the WCMSA.
For those workers’ compensation claims that were resolved on or after 6-1-10, and where the settlement includes non-covered Part D drugs as part of the WCMSA, CMS will consider a repricing of those cases that included non-covered Part D drugs. Once CMS performs a re-pricing of the WCMSA, beneficiaries may not use funds from their WCMSA to pay for non-covered Part D drugs. Doing so constitutes an inappropriate expenditure of WCMSA funds.
For those workers’ compensation settlements resolved on or after 6-1-10, and where the settlement does not include non-covered Part D drugs as part of the WCMSA, beneficiaries may not use funds from their WCMSA to pay for those non-covered Part D drugs. Doing so constitutes an inappropriate expenditure of funds from the WCMSA.
A87. All MSAs involving workers’ compensation settlements that occur on or after January 1, 2006 must include separate pricing for prescription drugs and medical services. If the workers’ compensation case did not settle prior to January 1, 2006 and the WCMSA proposal is received by CMS on or after January 1, 2006, then the submitter must include separate amounts for future medical treatment and future prescription drug treatment in the WCMSA proposal. For structured MSA proposals, the submitter must also indicate whether any portion of the future prescription drug treatment amount has been included in the initial deposit i.e., seed money. If the workers’ compensation claim was settled prior to January 1, 2006, the MSA did not need to specify a separate amount for future prescription drug treatment but rather allowed for prescription drug and medical services to be lumped together.
CMS’s policy regarding the pricing of prescription drugs did not change with the passage of this MMA. However, as of June 1, 2009 CMS requires that prescription drugs be priced using the average wholesale price as listed in RedBook® Drug Reference and makes it a standard practice to utilize the most current version of this resource when evaluating the sufficiency of the prescription drug component of a given MSA.
A88. No. If the workers’ compensation settlement included an allocation for non-Medicare covered medical and/or prescription drug expenses, the beneficiary must exhaust those funds prior to billing Medicare for prescription drugs assuming the beneficiary (a) has opted for Medicare Part D coverage or enrolled in a Medicare Part C plan that includes prescription drug coverage and (b) the beneficiary does not have any other coverage primary to Medicare.
A89. If the WCMSA proposal did not include an amount for future prescription drug treatment, and the current treatment records indicate that the beneficiary has been prescribed drugs and/or may need prescription drugs due to the work related injury or illness in the future, CMS will deem the submission as not adequately considering Medicare’s interests.
If the WCMSA did not include an amount for future prescription drug treatment, and there is no indication in the current treatment records that the beneficiary will need future treatment with prescription drugs related to the workers’ compensation injury, then CMS will accept that Medicare’s interests have been adequately considered. Medicare will then pay primary for future prescription drugs if the beneficiary has enrolled in a Medicare Part D prescription drug plan or Medicare Part C plan with prescription drug coverage and the beneficiary does not have any other coverage that is primary to Medicare.
A90. Yes. Beneficiaries who have not enrolled in either a Medicare Part D prescription plan or a Medicare Part C plan that includes prescription drug coverage need to include future prescription drug expenses in the WCMSA proposal if the current treatment records indicate that the beneficiary has been prescribed drugs and/or may need future prescription drug treatment related to the work or accident related injury or illness.
A91. Yes. Drug weaning commonly occurs with pain medications, such as opioids, especially when beneficiarys’ work injuries improve. The WCRC takes all evidence of drug weaning into account, although in most circumstances the WCRC cannot assume that the weaning process will be successful. Usually, the latest weaned dosage is extrapolated for the life expectancy, but again, they assess all records when making these types of determinations. Where a treating physician believes tapering is possible and in the best interests of the beneficiary, CMS will consider all evidence in making a WCMSA determination, including medical evidence of current actual tapering. See, WCMSA Reference Guide, §9.4.6.2.
A92. No. A previously submitted WCMSA proposal does not have to be resubmitted if CMS has already issued a written opinion as to the total WCMSA amount for settlements occurring prior to January 1, 2006. Note, if the workers’ compensation settlement occurred prior to January 1, 2006, and the workers’ compensation settlement included an allocation for future prescription drug treatment, then the beneficiary must exhaust those funds before Medicare can be billed for those future prescription drugs.
A93. Patents for brand name medications do expire and less expensive generic equivalents do usually become available thereafter. On the other hand, new more expensive brand name drugs often replace drugs whose patents are expiring. Finally, beneficiaries or their treating physician may insist on brand name drugs even where generic is available. All of these, along with the evidence submitted in a particular case, will be considered by CMS in determining the sufficiency of a proposed MSA amount.
A94. Off-label use of medications in the United States is both legal and common. Once a drug has been approved for sale by the FDA for one purpose, physicians are free to prescribe it for any other purpose that in their professional judgment is both safe and effective. Physicians are not limited to prescribing a drug only for official FDA approved indications.
For a drug to be covered under the Medicare Prescription Part D or Medicare Advantage Part C plan which includes prescription drug coverage, and thus included in a MSA, it must be used for a medically accepted indication. A medically accepted indication is any use for a covered outpatient drug which is approved by the FDA, or a use which is supported by one or more citations included or approved for inclusion in the recognized compendia.
Off-label use is when a drug is prescribed in a manner that is different from the FDA approved product labeling. There are many off-label indications that are listed in recognized compendia, and thus would be covered under the Medicare Prescription Part D or Medicare Advantage Part C plan which includes prescription drug coverage, and so should be included in a WCMSA.
See, WCMSA Reference Guide, §9.4.6.2.
A95. Where submitters furnish utilization review reports indicating that a beneficiary should be taking none, fewer, different, or less frequent drugs, this evidence will be considered by CMS. Reports of actual drug use from treating physicians will be given more weight than utilization review reports.
Conflicts between State & Federal Laws
A96. Medicare will generally honor judicial decisions issued after a hearing on the merits of a case by a court of competent jurisdiction or state Workers’ Compensation Commission. If a court or other adjudicator of the merits specifically designates funds to a portion of a settlement that is not related to medical services or prescription drug charges (e.g., lost wages), then Medicare will accept that designation.
“When a state WC judge approves a WC settlement after a hearing on the merits, Medicare generally will accept the terms of the settlement, unless the settlement does not adequately address Medicare’s interests. If Medicare’s interests were not reasonably considered, Medicare will refuse to pay for services related to the WC injury (and covered and otherwise reimbursable by Medicare) until such expenses have exhausted the dollar amount of the entire WC settlement. Medicare also will assert a recovery claim if appropriate. …If a court or other adjudicator of the merits (e.g., a state WC board or commission) specifically designates funds to a portion of a settlement that is not related to medical services (e.g., lost wages), then Medicare will accept that designation (emphasis added).” See, WCMSA Reference Guide, §4.1.4.
“A court order is “on the merits” when it is “delivered after the court has heard and evaluated the evidence and the parties’ substantive arguments.” Black’s Law Dictionary 1199 (9th ed. 2009)
However, a distinction must be made where a court or other adjudicator is only approving a settlement that incorporates the parties’ settlement agreements. Medicare will not accept the terms of the settlement as to an allocation of funds of any type if the settlement does not adequately consider Medicare’s interests. If Medicare’s interests are not adequately considered, Medicare will refuse to pay for medical services or prescription drug charges due to the work or accident related that are payable or otherwise reimbursable by Medicare until such expenses have exhausted the amount of the entire settlement. Medicare will also assert a recovery claim, if appropriate. See, WCMSA Reference Guide, §4.1.4.
A97. If a copy of the applicable statute is made part of the MSA submission to CMS then CMS will consider any statutorily defined non-compensable medical services or body parts/systems and evaluate any special situations. The practitioner is well advised to submit the applicable statute relied upon and present argument as to why the statute should be deciding on the issue.
Ethical Considerations
A98. Attorneys should consult their national, state, and local bar associations for information regarding their ethical and legal obligations. Additionally, attorneys should review applicable statutes and regulations, including, but not limited to 42 C.F.R. 411.24(e) and 42 C.F.R. 411.26.
At the very least the attorney must advise his or her client of the consequences of the client’s obligations under a self-administered MSA including the MSA funding (lump sum or structure) options, payment processes from the MSA, what future medical services and prescription drug charges will be payable under the MSA, what accounting obligations the client is assuming in the administration of the MSA, and what the client’s obligations are under the Medicare Secondary Payer Act regarding repayment of any conditional Medicare payments.
CMS is fond of using the term “protect” Medicare’s interests. An attorney’s obligation is to the client to insure the client understands Medicare rules and regulations as they apply to MSAs. It is not the attorney’s obligation to “protect” Medicare, rather the attorney’s obligation is to consider Medicare’s interest and in so doing protect the client’s interests.
A99. There are a number of areas the attorney needs to discuss with the client and document in the client’s file and these include:
- a. Settlement documents. These are not boilerplate documents and each is tailored to the individual fact pattern of each case to include provisions dealing with social security offset, MSA (self-administered or professional administration), MSA terms and conditions including accounting responsibilities, and any repayment obligations to Medicare or other entities that may have recovery rights
- b. Informed Consent. The client must make an informed consent as to the implications the settlement will have on future entitlement to Medicare, Medicaid, group health insurance or other available health coverage, short/long term disability coverage or pension plans, etc
- c. Notice of Consequences of the Settlement. The client must understand the entire settlement as to past, current or future indemnity, as well as, medical benefits and any repayment obligations which must be paid from the settlement.
- 4. Other documents provided by CMS. CMS will provide a sample accounting form to be used by the beneficiary in a self-administered Medicare Set-aside, as well as, an instruction sheet for either a self-administered or professionally administered MSA. These should be reviewed with the client as they are important disclosure documents which memorize the client’s obligations, expectations and responsibilities.
Sample documents are discussed and displayed in the Author’s text entitled Practitioner’s Reference Manual To Settlements, Offsets & Set-asides-Second Edition published by Atlantic Law Book Company, West Hartford, Connecticut 06110 as discussed in the overview of this Q & A. The reader is encouraged to visit: www.atlanticlawbooks.com/practionersGuide.htm.
.

